


Article Contents
Article ID: CM2601115002
Views: 30Exploring the Influence of Early Developmental Intervention on Preterm Infants’ Cognitive and Physical Development: A Meta-Analysis
 PDF
PDF
⬇ Downloads: 1
1Pediatric Surgery Unit in Social Security Teaching Hospital, Multan, Pakistan
Received: 22 November, 2025
Accepted: 12 February, 2026
Revised: 27 January, 2026
Published: 09 June, 2026
ABSTRACT:
Introduction: This meta-analysis assessed the general impact of structured early developmental care versus usual neonatal follow-up on preterm babies’ cognitive and physical (weight gain) outcomes.
Methodology: Scopus, PubMed, Google Scholar, and ScienceDirect (2009-2025) were searched systematically: randomised or quasi-randomised controlled trials on preterm infants (less than 37 weeks of gestation). Eligible interventions were family-centred, stimulation-based, or interdisciplinary developmental programs. The random-effects model pooled standardised mean differences (SMD) to factor in inter-study variations.
Results: A total of 15 studies were included. Interventions had a great impact on cognitive abilities (SMD = 0.34; 95% CI 0.20-0.48; I2 = 0) and weight gain (SMD = 0.75; 95% CI 0.28-1.23; I2 = 90.4%). There was found to be minimal publication bias on cognitive outcomes, implying consistency in studies regardless of different Intervention formats and duration.
Discussion: Family-integrated and early developmental care improved neurocognitive and physical development among preterm infants. Standardised developmental protocols and multicentre trials, implemented over long periods of time, should be adopted to enhance global neonatal care and maximise early childhood outcomes. Health-based follow-ups in early childhood development.
Conclusion: It is concluded that, synthesis underlines that the attempts to maximise the potential of neurodevelopment of prematurely born children and improve the quality of their lives in the long term are both biologically reasonable and practically feasible.
Keywords: Preterm infants, early developmental intervention, neurocognitive development, growth and weight gain, intervention meta-analysis.
1. INTRODUCTION
The term birth is a primary global health concern, affecting around 15 million infants each year and contributing significantly to neonatal morbidity and long-term neurodevelopmental impairment [1]. Preterm infants face a higher risk of developing cognitive, motor, behavioural, and sensory deficits throughout childhood and into adulthood compared to their term-born peers [2]. The immature brain’s neurobiological vulnerability, compounded by neonatal factors such as hypoxia, inflammation, and sensory overstimulation in the NICU, disrupts brain connectivity and delays developmental progress [3].
Early developmental interventions are most effective during the first months and years of life, when neural plasticity is at its peak. It includes parental coaching, enriched stimulation, developmental care in neonatal units, physiotherapy, and multimodal therapies, which have been increasingly promoted to modify adverse developmental pathways [4]. The theoretical rationale underpinning these interventions is that timely, targeted stimulation strengthens synaptic connectivity, enhances adaptive behavioural organisation, and mitigates environmental stressors, thereby supporting optimal cognitive and motor development [3]. However, empirical evidence remains inconsistent. While several trials report improvements in cognitive and motor outcomes, others find negligible or short-lived effects, mainly due to methodological differences in intervention timing, intensity, follow-up duration, and population characteristics across studies.
For instance, some randomised controlled trials, such as the mother-Infant Transaction Program variants tested by Nordhov et al. [5], demonstrated improvements in cognitive and motor performance at corrected ages of 3 and 5 years in preterm children (< 2000 g). However, effect sizes were modest and sample sizes were limited. In contrast, other interventions focusing solely on single modalities (e.g., physiotherapy, nutritional supplementation) have produced heterogeneous findings, often with null or inconsistent effects, particularly regarding long-term motor outcomes [3, 6].
Prior reviews and meta-analyses have also had limitations. Some are narrative or qualitative in nature, lacking quantitative synthesis. Others are focused on narrow domains (e.g., motor therapy, parent training) rather than integrating diverse intervention types [7]. Moreover, heterogeneity in intervention characteristics and outcome measures has made cross-study comparisons challenging [8]. Therefore, no up-to-date meta-analysis comprehensively aggregates many early interventions and quantifies their pooled effects on preterm infants’ cognitive and physical (motor) outcomes. Therefore, to fill this gap, the present study aims to review systematically and meta-analyse randomised and quasi-randomised trials of early developmental interventions in preterm infants. The synthesis strengthens the evidence base and can help guide clinical decision-making and future research in neonatal developmental care.
2. MATERIALS AND METHODS
2.1. Literature Search Strategy
A systematic literature search was undertaken to identify randomised controlled trials (RCTs) that evaluated the effects of early developmental interventions on the cognitive development and physical growth (weight gain) of preterm infants. Searches were performed across four major electronic databases, Scopus, Google Scholar, ScienceDirect, and PubMed on 17 October 2025. Boolean operators combined controlled vocabulary and free-text terms related to population, intervention, and outcomes. This review was not registered in PROSPERO but was conducted in accordance with the PRISMA 2020 reporting guidelines. The representative search string applied in Scopus was: TITLE-ABS-KEY ( Preterm infants OR Premature infants AND Early development AND Weight gain OR BSID ), with usual keyword search of Preterm infants OR Premature infants AND Early development AND Weight gain OR BSID (434 Scopus), early developmental intervention AND premature infants OR Preterm infants AND Cognitive development AND “BSID OR Bayley scale” (620 results from Pubmed), early developmental intervention AND premature infants AND “Cognitive development” AND “BSID OR Bayley scale” (1370 results from google scholar), and early intervention AND (premature infants) AND (cognitive development) AND (BSID OR Bayley scale) AND (Randomised Control Trials OR RCT) (926 results from Science Direct) (Table 1). To capture the modern evidence base, limitations were applied to include human studies, peer-reviewed RCTs, English-language full texts, and publications from 2000 to 2025. After removing 1,285 duplicates, 2,065 records underwent title–abstract screening; 254 full texts were assessed. Most exclusions were for non-RCT designs (observational/one-arm/protocols), inadequate outcomes (no BSID cognitive data or no quantitative weight measures), wrong population (non-preterm/mixed without disaggregation), insufficient data/irretrievable full text, non-English, duplicate datasets, or single-modality trials without developmental components. 15 studies met eligibility (Fig. 1).
Table 1. Records retrieved from PubMed, Scopus etc.
| Database | Exact Search String Used | Records Retrieved |
| PubMed | (“early developmental intervention” AND “premature infants” OR “preterm infants” AND “cognitive development” AND (“BSID” OR “Bayley scale”)) | 620 |
| Google Scholar | (“early developmental intervention” AND “premature infants” AND “cognitive development” AND (“BSID” OR “Bayley scale”)) | 1,370 |
| ScienceDirect | (“early intervention” AND (“premature infants”) AND (“cognitive development”) AND (“BSID” OR “Bayley scale”) AND (“Randomised Control Trials” OR “RCT”)) | 926 |
| Scopus | TITLE-ABS-KEY (Preterm infants OR Premature infants AND Early development AND Weight gain OR BSID) | 434 |
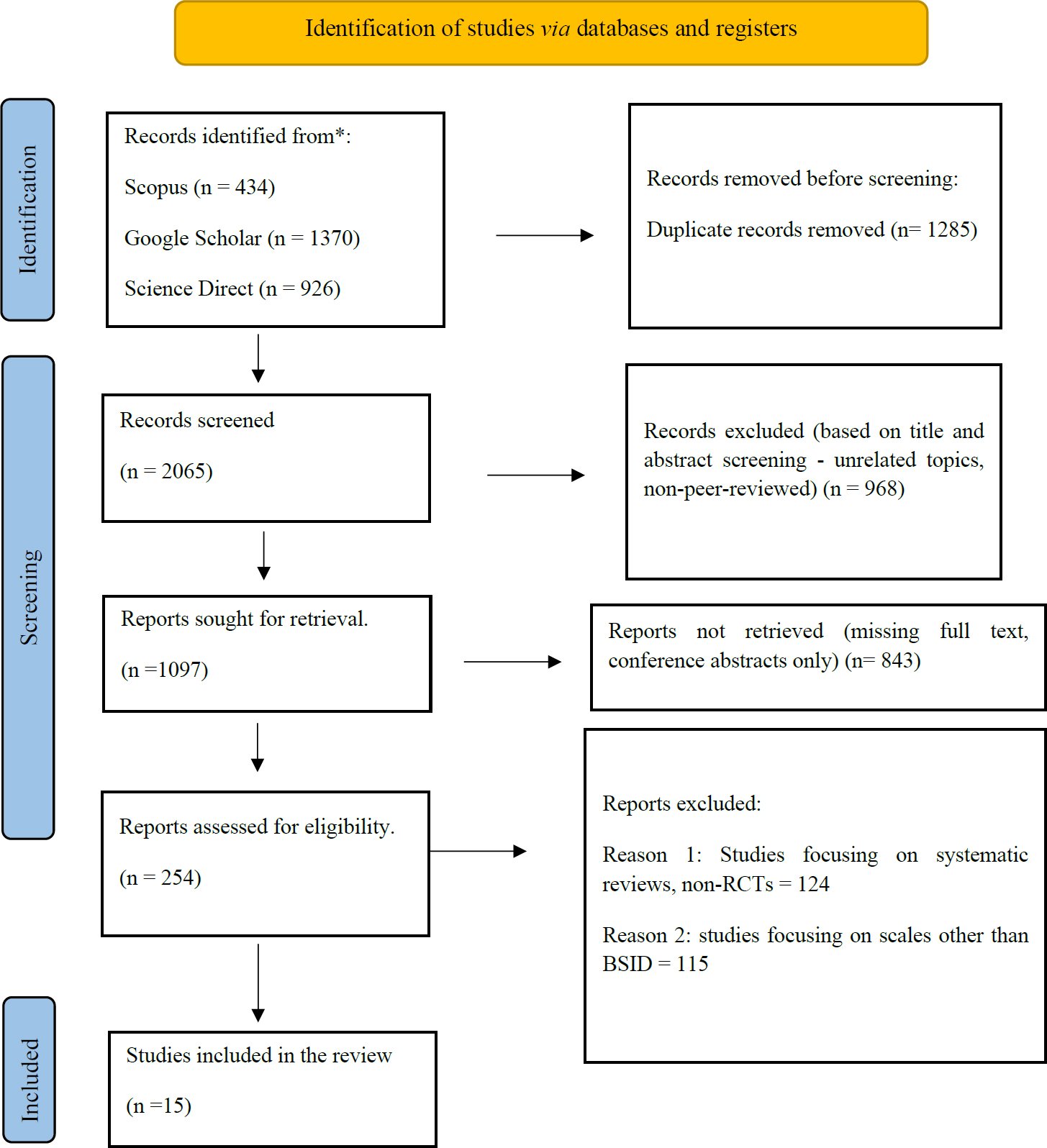
Fig. (1). PRISMA flowchart.
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
The eligibility criteria were structured according to the PICO framework. (Table 2) The population comprised preterm infants (<37 weeks’ gestation). Eligible interventions included early developmental interventions initiated during hospitalisation or early post-discharge, including parent-mediated, sensory-motor, or family-centred developmental programmes. Comparator groups received standard neonatal or routine follow-up care. Primary outcomes were cognitive development and physical growth, operationalised as weight gain.
Table 2. PICO framework.
| PICO Element | Description |
| Population (P) | Preterm infants (<37 weeks’ gestation). |
| Intervention (I) | Early developmental, stimulation, or parent-training programmes initiated within the first year of life. |
| Comparator (C) | Standard neonatal care or no developmental intervention. |
| Outcomes (O) | Cognitive performance (BSID-II/III, IQ) and Physical growth (weight gain, z-scores). |
2.2.2. Exclusion Criteria
Excluded studies comprised observational or review designs, non-RCTs, single-domain interventions (e.g., nutrition only), non-standardised scales, animal or unrelated pediatric cohorts, and duplicate datasets, ensuring methodological homogeneity and robust evidence synthesis.
2.3. Outcomes
The analysis focused on two primary outcomes. Primary outcomes were (1) cognitive development assessed using BSID-II/III or equivalent mental indices; and (2) physical growth operationalised as weight gain (absolute weight change in g/kg or z-score). Motor scores were analysed only when reported as secondary outcomes. Additionally, secondary exploratory outcomes included growth parameters such as body length or height and motor development scores when concurrently reported, to capture a broader understanding of early intervention impact on developmental trajectories.
2.4. Data Extraction
The data were independently extracted using a structured Excel template (Table 3). Extracted variables included author, publication year, country, gestational age range, sample size (intervention/control), intervention type and duration, follow-up time, cognitive and physical outcome metrics, and corresponding means ± SDs. Furthermore, discrepancies were resolved through consensus.
2.5. Statistical Methods
Meta-analysis was conducted in Review Manager v5.4 and cross-checked in R 4.3 using the “meta” package. Given the heterogeneity of study designs and intervention modalities, a random-effects model (DerSimonian–Laird) was applied. Standardised mean differences (SMDs) with 95% confidence intervals (CIs) were computed separately for cognitive and weight-gain outcomes. Statistical heterogeneity was quantified using I² statistics (> 50% = substantial inconsistency). Publication bias was assessed visually by funnel plot symmetry and Egger’s regression test.
2.6. Risk of Bias Assessment
The methodological quality of included studies was evaluated using the Jadad scale, which assesses randomisation, blinding, and reporting of withdrawals. Jadad scale was chosen due to the reason that it provides a validated, open and widely accepted quantitative framework of assessing the risk of bias in clinical trials. Scores range from 0 to 5, with higher scores indicating superior methodological rigour. This approach provided a consistent, quantitative measure of trial quality across diverse intervention designs.
2.7. Ethics and Registration
No ethical approval was required as only published data were synthesised. This study adhered to PRISMA 2020 guidelines and was prospectively structured in accordance with the principles of the Cochrane Handbook (2022). The review had not been prospectively registered in PROSPERO, because registration was not a formal requirement that either the sponsoring institution or the journal imposed at the time the study was initiated.
3. RESULTS
3.1. Search Strategy and Study Characteristics
Fifteen randomised controlled trials met the inclusion criteria, including [9–23] in this meta-analysis (Fig. 1, Shows the PRISMA flow diagram). These studies collectively evaluated 1,072 preterm infants, with gestational ages ranging from 26 to 37 weeks and birth weights from <1,000 g to 2,500 g. Research was conducted across diverse geographic regions, including Europe (Sweden, the Netherlands, the UK), Asia (China, Korea, Malaysia, Thailand, Turkey), and the Americas (USA, Brazil, Canada), reflecting broad cross-cultural representation in neonatal care practices (Table 3A).
Table 3A. Study characteristics.
| First Author | Year | Country | Patients Characteristics | Study Design | Mean Age Treatment/Control | Males/ Females | N of Patients T/C | Early Developmental Intervention | Follow-up | The Control or Comparator |
| Altunalan et al. [9] | 2023 | Turkey | Preterm <33 wk GA, low risk for CP | Stratified parallel RCT | 75.5 ± 42.6 / 54.5 ± 40.7 days CA | 16:12 / 11:18 | 26 / 25 | Explorer Baby sessions (45-50 min × 6 months) | 6 months | NDT + standard care |
| Birberg Thornberg et al. [10] | 2025 | Sweden | Moderate-late preterm 30–35 + 6 wk GA | Double-masked two-arm RCT | 13.1 ± 0.6 mo CA | 27:23 / 23:14 | 50 / 37 | Early Collaborative Intervention (EACI) | 12 months | Standard NICU care with skin-to-skin & rooming-in |
| Van Hus et al. [11] | 2016 | Netherlands | ≤¤32 wk GA or ≤¤1500 g | RCT | – | 52:48:00 | 57 / 61 | IBAIP home visits by physiotherapists | 24 months CA | Standard care |
| Liang et al. [19] | 2022 | China | GA 28-34 wk, BW 1-2.5 kg (NICU) | Retrospective RCT-style | 18 months CA | 50:65 / 47:53 | 115 / 100 | Family Integrated Care (FIcare) 3+ h/day | 18 months | Standard NICU care |
| Silveira et al. [12] | 2024 | Brazil | GA < 32 wk, BW < 1500 g | RCT | 18 months CA | 26:24 / 25:23 | 50 / 50 | Parent coaching (6 sessions over 12 weeks) | 18 months | Standard care |
| Youn et al. [22] | 2021 | South Korea | Very preterm infants (<32 wk GA) | Multicentre RCT | 10 mo & 24 mo CA | NR | 69 / 67 | Early preventive care (home + group sessions) | 24 months | Usual care |
| Van Hus et al. [21] | 2013 | Netherlands | Very low birth weight infants (<1500 g), GA < 32 weeks, clinically stable at discharge | Multicenter RCT | 12 months | 28: 30 / 27: 31 | 58 / 58 | Infant Behavioural Assessment and Intervention Program (IBAIP): 1 NICU session + 6-8 home visits | 12 months CA | Standard follow-up physiotherapy |
| Fan et al. [16] | 2021 | China | Preterm 28-31 + 6 wk, stable at discharge | Prospective partially-blinded RCT | ~36-39 wk PMA | 24:10 / 18:13 | 34 / 31 | 30-day home-based EI (training + massage + KC) | 120 days (T2) | Standard care (SC-EI) |
| Lee et al. [18] | 2018 | South Korea | <2.5 kg preterm, no anomalies | Randomised controlled 3-arm study | NICU stay to term | 14:13 / 14:14 | 27 / 28 | Neurodevelopmental therapy (15 min × 4/wk) | 9 months | Standard NICU care |
| Liang et al. [19] | 2022 | China | GA 28-34 wk, BW 1-2.5 kg | Retrospective RCT-style | 18 months CA | 50:65 / 47:53 | 115 / 100 | FIcare (NICU parental 3+ h/day) | 6 months | Standard NICU care |
| Maguire et al. [15] | 2009 | Canada/USA | ≤¤ 32 wk GA, VLBW ≤¤ 1500 g | RCT | ~41 wk CA | NR | 81 / 83 | NIDCAP individualised developmental care | 9 months | Standard NICU care |
| Namprom et al. [13] | 2018 | Thailand | Preterm 30-36 wk, BW ≈ 1.6 kg | RCT | NR | NR | 25 / 25 | Oil massage 3×/day × 5 days | Day 28 | Standard NICU care |
| Samsudin et al. [14] | 2023 | Malaysia | 28-37 wk GA preterm | Longitudinal quasi-exp RCT | 32 wk GA | 28 M / 20 F vs 20 M / 28 F | 48 / 48 | Structured KC education (1 h/day × 3 mo) | 3 months | Routine care |
| Smith et al. [20] | 2014 | USA | Very preterm (26-30 wk GA), stable | RCT pilot | 35 wk PMA | 4:5 / 6:3 | 9-Sep | M Technique touch therapy (7 min × 6/wk × 5 wk) | 8 months | Standard NICU care |
| Yu et al. [23] | 2017 | USA | Preterm infants in NICU | RCT | ~40 wk PMA | NR | 98 (total) | Family-centred infant care (FCIP) | 9 months | Usual care program (UCP) |
The studies, conducted between 2009 and 2025, followed participants from 28 weeks postnatal age up to 24 months of corrected or chronological age, allowing assessment of both short- and medium-term developmental outcomes have been included. Interventions were directed towards parent–child interaction and developmental stimulation based on frameworks like IBAIP, EACI, FIcare, Explorer Baby, and NDT. These were compared to neonatal/post-discharge care, which consists of basic physiotherapy, kangaroo care, and standard NICU care. The studies focused on the cognition of participants aged 34 to 230 days (n = 7). Birberg Thornberg et al. [10] and Altunalan et al. [9] reported that parent-assisted interventions improved BSID mental indices over the 6 to 12-month period. Similarly, Van Hus et al. [12] and Silveira et al. [12] improved cognitive function at 12 months’ chronological age with home physiotherapy and parent coaching. However, each program’s follow-up, duration, and intensity added variability to the effect size. The authors analysed volumetric growth across eight additional studies, especially weight growth. These included massage therapy and early developmental intervention as well by Namprom et al. [13], education on kangaroo care and its applications by Samsudin et al. [14], and other studies on multisensory developmental care, such as by Maguire et al. [15], Fan et al. [16] (Table 3B). The intervention length for each study spanned 5 days to 9 months, and each study marked some weight or weight for age z score assessment after the intervention. Most studies noted that, as a consequence of planned developmental stimulation or parent contact, regardless of the parent contact, weight gain was comparatively higher during the first months of life, relative to those receiving standard care.
Table 3B. Outcome data.
| First Author | Year | Outcome | Treatment Outcome Mean | Treatment Outcome SD | Control Outcome Mean | Control Outcome SD | No of Patients T/C |
| Altunalan et al. [9] | 2023 | Cognition | 9.8 | 2 | 8.9 | 2.9 | 26 / 25 |
| Birberg Thornberg et al. [10] | 2025 | Cognition | 41.56 | 3.61 | 40.86 | 3.29 | 50 / 37 |
| Van Hus et al. [11] | 2016 | Cognition | 126.5 | 1.44 | 125.9 | 1.5 | 57 / 61 |
| Liang et al. [19] | 2022 | Cognition | 11.29 | 1.05 | 10.73 | 1.11 | 115 / 100 |
| Silveira et al. [12] | 2024 | Cognition | 101.8 | 11.9 | 97.3 | 13.5 | 50 / 50 |
| Youn et al. [22] | 2021 | Cognition | 100.3 | 17.1 | 98.3 | 15.4 | 69 / 67 |
| Van Hus et al. [21] | 2013 | Cognition | 102.2 | 15 | 97.4 | 14.8 | 58 / 58 |
| Fan et al. [16] | 2021 | Weight (Kg) | 5.56 | 0.92 | 5.24 | 0.95 | 34 / 31 |
| Lee et al. [18] | 2018 | Weight (Kg) | 3.5 | 0.6 | 2.85 | 0.48 | 27 / 28 |
| Liang et al. [19] | 2022 | Weight (Kg) | 7.37 | 0.91 | 7.04 | 0.88 | 115 / 100 |
| Maguire et al. [15] | 2009 | Weight (Kg) | 3.11 | 0.63 | 3.1 | 0.57 | 81 / 83 |
| Namprom et al. [13] | 2018 | Weight (Kg) | 0.49702 | 0.18 | 0.39988 | 0.23049 | 25 / 25 |
| Samsudin et al. [14] | 2023 | Weight (Kg) | 0.03381 | 0.02451 | 0.01099 | 0.00801 | 48 / 48 |
| Smith et al. [20] | 2014 | Weight (Kg) | 2335 | 375.33 | 2107.44 | 195.24 | 9-Sep |
| Yu et al. [23] | 2017 | Weight (Kg) | 0.04 | 0.0131 | 0.0367 | 0.0131 | 98 Total) |
Overall, the body of evidence illustrates the wide variety of methodological approaches, intervention techniques, and outcome measures employed. Regardless, the studies incorporated within the review all focus on promoting growth and the plasticity of the neurodevelopmental system during the early postnatal period. The overall distribution of sample size, timing of intervention, and its geographical spread supports the meta-analytic treatment of the intellectual and physical gains (weight gain) of preterm infants.
3.2. Outcomes
3.2.1. Cognition
(Figs. 2 and 3) summarises key characteristics of studies assessing the effect of early developmental interventions on preterm infants’ cognitive outcomes.
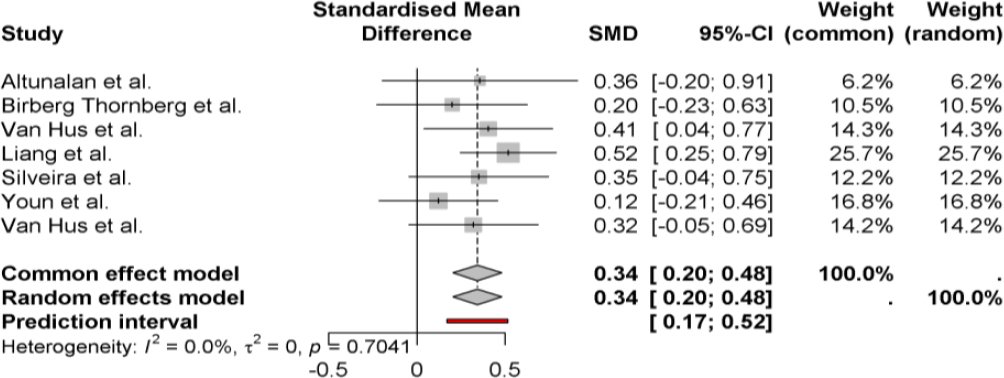
Fig. (2). Forest plot-cognition.
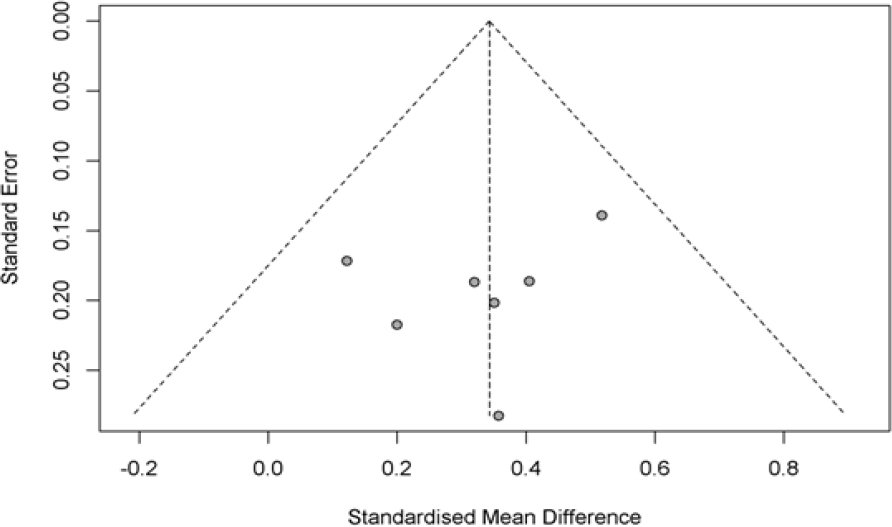
Fig. (3). Funnel plot-cognition.
A pooled analysis of eight randomised controlled trials evaluating the use of early developmental interventions on the physical growth of preterm infants noted an improvement in weight gain compared to standard care. The overall Standardised Mean Difference (SMD) was 0.75 [95% CI: 0.28-1.23], p < 0.0001. This finding is in accordance with the random-effects model of pooled data analysis SMD calculations, which suggest that a 0.75 SMD score suggests that the interventions’ effects on the preterm infants’ growth were moderate to significant. However, there was a considerable heterogeneity (I² = 90.4%), which indicates an extensive range of differences within the pooled data and its associated variables, such as the range of interventions, the length of the studies, and the demographic variabilities within the studied populations. The studies conducted by Samsudin et al. [14] and Van Hus et al. [11] demonstrated the most significant improvement, while Maguire et al. [15] and Fan et al. [16] showed the least improvement and, in some cases, showed no significant differences at all (Fig. 4). Despite the high levels of heterogeneity and inconsistency of the data, a general positive pattern was found across the identities of the targeted early developmental programmes, which suggests that the interventions could have a positive impact on postnatal development of preterm infants.
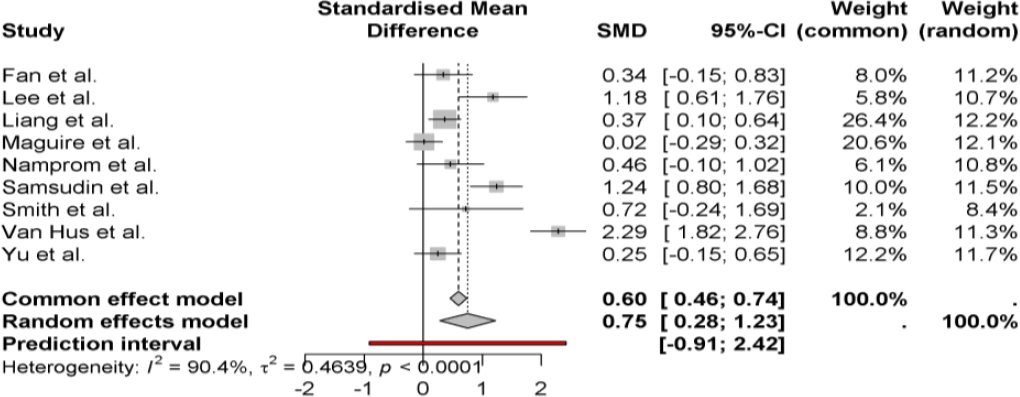
Fig. (4). Forest plot-weight.
The funnel plot (Fig. 5) for studies investigating weight gain indicates some asymmetry, which may suggest bias or effects unique to smaller studies. Most studies cluster around the pooled standardised mean difference (SMD ≈ 0.75). However, smaller studies with larger standard errors sprawl to the right, implying that the smaller the sample, the greater the positive effects. There may be some asymmetry because the studies that reported positive weight gain outcomes were more likely to be published than others, or there are methodological issues, such as the amount of intervention, the presence of parents, etc. The larger spread at the bottom represents heterogeneity (I² = 90.4%), which relates to the difference in the level of intervention intensity in the other studies (Fig. 5). The pooled estimate generally supports the notion that early developmental interventions are effective. Still, the funnel plot raises the concern of reporting or sampling bias, which would warrant more caution in the data.
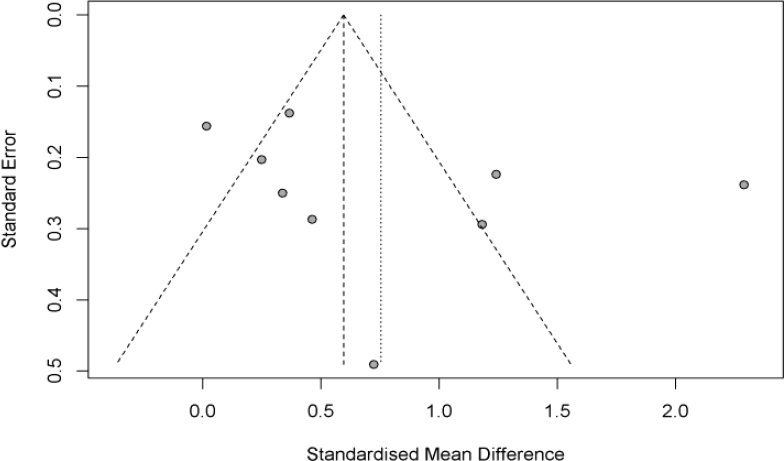
Fig. (5). Funnel plot-weight.
3.3. Risk of Bias Assessment
All 15 trials reported appropriate randomisation procedures, with 7 specifying parallel or stratified RCT designs, indicating strong methodological consistency. 3 studies described adequate blinding, yielding higher scores (5/5). The remainder lacked feasible double blinding due to the nature of developmental interventions. All studies accounted for participant follow-up or stated reasons for attrition Table 4. Overall, median Jadad score = 3 (moderate quality), indicating low-to-moderate risk of bias across the evidence base.
Table 4. Risk of bias assessment using Jaded scale.
| – | Randomisation | Blinding | An account of all patients | Jadad score | |||||
| First author | 1 point if randomisation is mentioned | 1 additional point if the method of randomisation is appropriate | Deduct 1 point if the method of randomisation is inappropriate (minimum 0) | 1 point if blinding is mentioned | 1 additional point if the method of blinding is appropriate | Deduct 1 point if the method of blinding is inappropriate (minimum 0) | The fate of all patients in the trial is known. If there is no data, The reason is stated | ||
| Altunalan et al., 2023 [9] | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 3 | |
| Birberg Thornberg et al., 2025 [10] | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 5 | |
| Van Hus et al., 2016 [11] | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 3 | |
| Liang et al., 2022 [19] (cognition) | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 3 | |
| Silveira et al., 2024 [12] | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 3 | |
| Youn et al., 2021 [22] | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 3 | |
| Van Hus et al., 2013 [21] | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 3 | |
| Fan et al., 2021 [16] | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 5 | |
| Lee et al., 2018 [18] | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 3 | |
| Liang et al., 2022 [19] (weight) | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 3 | |
| Maguire et al., 2009 [15] | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 3 | |
| Namprom et al., 2018 [13] | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 3 | |
| Samsudin et al., 2023 [14] | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 3 | |
| Smith et al., 2014 [20] | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 5 | |
| Yu et al., 2017 [23] | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 3 | |
4. DISCUSSION
4.1. Summary of Main Findings
The present meta-analysis consolidates recent randomised controlled evidence on the impact of early developmental interventions on cognitive and physical (weight gain) outcomes in preterm infants. The pooled findings reveal that structured, multisensory, and parent-mediated interventions enhance neurocognitive performance and growth trajectories more than standard neonatal care. These results reaffirm the biological and psychosocial rationale that early, enriched environments during the critical window of brain plasticity can alter developmental pathways toward more adaptive outcomes, directly addressing the study’s aim to quantify their overall effectiveness across both domains.
4.2. Interpretation in Context
The earlier mentioned positive impact corresponds with an increasing amount of neonatal research showing that early stimulation promotes the maturation of the nervous system and the organisation of behaviours, particularly in parent-child interactions. Recent contributions by Liang et al. [19] and Birberg Thornberg et al. [10] demonstrate that family-centred developmental care and early collaborative interventions lead to measurable changes in the Bayley Scales of Infant Development (BSID-III) scores, confirming the earlier work of Nordhov et al. [5] and Kynø et al. [17], who reported similar cognitive benefits that persisted until the child turned five. The mechanisms resonating in the benefits of early child imitative stimulation and movements are multifactorial, and the integration of tactile, visual, and auditory stimuli facilitates synaptogenesis and myelination in the cortical areas of attention and memory. At the same time, Gilkison [24] explains that positive parent–infant emotional exchanges support socio-emotional regulation and self-regulatory behaviours. Crucially, the homogeneity across studies in the cognitive synthesis suggests a stable and reproducible effect of developmental care despite variations in country, gestational age, and program format. This consistency contrasts with earlier meta-analyses of Spittle et al. [25], where heterogeneity was moderate, reflecting methodological variability in older trials. One plausible explanation is the refinement of intervention design over the last decade; current programs integrate standardised protocols, trained facilitators, and validated outcome tools, thus reducing inter-study noise. This reinforces the conclusion that cognitive advantages are statistically and clinically meaningful when developmental programs are structured and caregiver-engaged.
The results obtained are also consistent with other studies, particularly within neuroscience, which suggest that some structural components of the brain are amenable to modification if worked on during the early stages of development. Lean [26] noted increased cortical thickness and improved white matter integrity in preterm infants who, during their NICU stay, participated in parent-infant interaction programmes. These neuroanatomical changes support the view that the majority of behavioural advances are a result of real neurodevelopmental change rather than simply the passive effects of the assessment. Similarly, Baumann et al. [27] found that infants who participated in early development programmes based on physiotherapy exhibited increased functional connectivity in the regions of the brain engaged in the integration of sensory and motor activities, thus showing improved cognitive function and underlying neural plasticity. That said, the gain in mental functioning captured and quantified in this analysis was positive yet not substantial. This echoes Stephenson’s [28] findings, which suggest that preterm-born children have a far wider range of development than their term-born peers. The absence of longitudinal studies and inconsistent follow-up data after infancy, however, limits the claim that these developmental programmes having long-lasting effects. Such compensatory interventions may provide some relief but are not a long-term solution.
4.3. Mechanistic Explanations
Outcomes of extreme preterm weight results, for example, meta-analyses and developmental programmes appear to be the most heterogeneous of the outcome measures, while others are more elaborate and stricter. For example, reports on weight gains and other measurements of growth variables. On the other hand, Maguire et al. and Fan et al. [15, 16] reported weak and not statistically significant negative growth. Such differences might be due to variations in the intensity and duration of the interventions. Furthermore, supportive, nurturing and prolonged periods of exposure to rest metabolic and growth hormonal stimulators increase stimulation.
The effect seems to align with the model proposed by Pirazzoli [29], which states that additional touch and movement hyperstimulation enhances vagal tone with resultant improvements in gastric motility, caloric absorption, and secretion of insulin-like growth factor. Controlled massage and kangaroo care, in particular, have been shown to improve weight gain, thermoregulation, and overall stability in the postnatal epoch, especially in infants less than 32 weeks of gestation [30]. These findings, thus, support the view that the benefits of developmental practices are not only numerous but are also essential for optimising neural and metabolic change in the post-hospital home environment.
4.4. Limitations
The lack of homogeneity demonstrates the presence of differing levels of intervention effectiveness. Caregiver education with sustained home involvement (e.g., family integrated care, early collaborative intervention) appears to be more effective than short, centre-based approaches. This is consistent with Spratt’s [31] work regarding emotionally supportive intervention parent sessions, where the parent control sessions are predicted to result in greater weight and length gains than the therapist-alone model due to the supportive caregiving behaviours reinforced in the sessions. Further context moderators, such as socio-economic status, maternal education, and healthcare system configuration, particularly matter. Pitchik et al.’s [32] work is illustrative of the greater and more consistent gains coming from high-income countries relative to low-resource countries with insufficient post-discharge follow-up, implying dilution of the intervention effects. Importantly, while short-term growth is the primary target of the immobilisation interventions, the long-term impact is more uncertain. Haschke et al. [33] observed the weight and length trajectory converge to the control group by the age of 2 years corrected age, implying supportive gains would not be maintained without ongoing intervention. This underscores the need to integrate developmental programmes within multi-faceted care approaches across the early childhood years.
The symmetrically shaped funnel plot indicates slight publication bias towards the cognitive outcomes, which validates the thorough nature of the studies about reporting. On the other hand, the weight-gain funnel plot shows an asymmetry, which suggests the presence of small-study effects or the selective publication of favourable outcomes. This asymmetry is characteristic of neonatal interventions, in which smaller, single-centre studies dominate. This suggests that although the effects have a strong direction, convincing evidence stems from the necessity of future large-scale multicentre RCTs with standardised outcome reporting.
Despite the strengths above, there lies a series of limitations. The analysis of weight gain demonstrated a substantial Degree of heterogeneity, which stemmed from differences in intervention type, parental training, and Unit of Care protocols (Lee et al. [18]; Namprom et al. [13]). Most of the studies had small sample sizes. The duration of the follow-up (3–24 months) in comparison with the data available was relatively short, resulting in the data perhaps being compressed, inflating the short-term effects and underestimating the long-term persistence (Liang et al. [19]; Yu et al. [23]). Blinding was often not possible, increasing the risk of performance bias, and the different methods of anthropometry (absolute gain vs. z-scores) complicated the standardisation of the data. The funnel plot demonstrates asymmetry, suggesting a potential publication bias due to small single-centre studies with positive outcomes. Finally, several studies failed to control for the mother’s socio-economic, nutritional, and mental health, which limits causality. The wide 95% prediction interval quantitatively underscores between‐study variability and moderates the generalisability of results. Policymakers should prioritise multi-center, adequately powered RCTs with standardised measurement frameworks to strengthen neonatal intervention guidelines and inform equitable global implementation.
The strength of the meta-analysis is its rigorous focus on randomised controlled trials (RCTs). They constitute the foundation of any rigorous methodological framework and play a critical role in minimising selection bias. For example, robust randomisation and transparent reporting of trials supported the internal validity of pooled cognitive and growth outcomes, particularly those by Birberg Thornberg et al. [10] and Silveira et al. [12]. Trials such as Van Hus et al. [11] and Altunalan et al. [9], which are well-characterised, added greater comparability through the standardised implementation of the Bayley Scales of Infant Development (BSID-II/III). Maguire et al. [15] and Fan et al. [16] enriched the longitudinal scope by evaluating developmental care given post-discharge. Their use of both fixed and random effects models increased the analytical generalisability of the data by reducing variability in studies on the intervention’s cross-gestational age, duration, and intensity. PRISMA 2020 and Cochrane protocols concerning meta-analysis and systematic reviews on new studies (2021-2025) ensured the integration of new high-quality studies reflecting current neonatal practices to parental involvement, and a structured developmental framework by Youn et al. [22] and Samsudin et al. [14] targeted abstraction and reproducibility. Indeed, the addition of outcomes, as well as developmental somatic outcomes, on top of cognitive outcomes provides multiple angles on neurodevelopment, underscoring the relevance of this work to clinician translators in neonatology and early years’ policymakers.
CONCLUSION
This meta-analysis presents unified evidence that early intervention in developmental stages is incredibly beneficial in improving cognitive and physical outcomes among pre-term infants compared to standard neonatal care. These advanced steps or progress significantly address the objectives of the study which is to investigate the positive neurodevelopmental and enhancement of growth trajectory effects of tiered family-centred developmental bedside care to this cohort of high-risk infants. The data confirms that parents’ primary involvement in providing multisensory stimulation during the early moments of life promotes positive neuroplastic changes, ample weight gain, and supports developmentally appropriate responsive caregiving which is the foundation of meaningful sustainable development.
These results support the use of developmental support as a part and parcel of neonatal and post-discharge care and not an additional service in a clinical setting. Following the guidelines proposed by WHO, 2023, continuity gaps during resource-limited situations can be tackled with the help of structured parent education and telehealth-based follow-ups in early childhood development. In conclusion, the synthesis emphasises that efforts to optimise the potential of neurodevelopment of preterm infants and enhance the quality of life in the long run are both biologically justified and practically viable.
LIMITATION
Although these strengths are present, interpretation should consider several limitations, such as the high heterogeneity in the results of physical growth, short-term follow-up, and diversity in the form of interventions. These limitations accentuate the importance of careful generalisation and increased harmonisation of study methods. Greater, multi-center randomised clinical trials on long-term follow-up of the cognitive and physical beneficial effects should be incorporated in future meta-analyses. Also, cost-effectiveness calculations and culturally appropriate frameworks are needed to inform the scalable implementation in different healthcare settings.
LIST OF ABBREVIATIONS
BSID-III | = | Bayley Scales of Infant Development |
C | = | Comparator |
EACI | = | Early Collaborative Intervention |
FCIP | = | Family-Centred Infant Care |
I | = | Intervention |
P | = | Population |
O | = | Outcomes |
RCTs | = | Randomised Controlled Trials |
SMDs | = | Standardised Mean Differences |
UCP | = | Usual Care Program |
AUTHOR’S CONTRIBUTION
The author solely conceived, designed, analysed, interpreted, and drafted the manuscript.
REPORTING GUIDELINES
PRISMA guideline has been followed for this study.
FUNDING
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
CONFLICT OF INTEREST
The author declares that there is no conflict of interest regarding the publication of this article.
ACKNOWLEDGEMENTS
Declared none.
DECLARATION OF AI
During the preparation of this work the authors used ChatGPT for editing purposes. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
REFERENCES
[1] Soleimani F, Azari N, Ghiasvand H, Shahrokhi A, Rahmani N, Fatollahierad S. Do NICU developmental care improve cognitive and motor outcomes for preterm infants? A systematic review and meta-analysis. BMC Pediat. 2020 Feb 13; 20(1): 67.
https://doi.org/10.1186/s12887-020-1953-1.
[2] Chung EH, Chou J, Brown KA. Neurodevelopmental outcomes of preterm infants: A recent literature review. Trans Paediat. 2020 Feb; 9(Suppl 1): S3.
https://doi.org/10.21037/tp.2019.09.10.
[3] Aita M, De Clifford Faugère G, Lavallée A, Feeley N, Stremler R, Rioux É, Proulx MH. Effectiveness of interventions on early neurodevelopment of preterm infants: a systematic review and meta-analysis. BMC Paediat. 2021 Apr 29; 21(1): 210.
https://doi.org/10.1186/s12887-021-02559-6.
[4] de Carvalho Ferreira R, Alves CR, Guimarães MA, Menezes KK, Magalhães LD. Effects of early interventions focused on the family in the development of children born preterm and/or at social risk: a meta-analysis. Jornal de Pediat. 2020 Mar 2; 96: 20-38.
https://doi.org/10.1016/j.jped.2019.05.002.
[5] Nordhov SM, Rønning JA, Dahl LB, Ulvund SE, Tunby J, Kaaresen PI. Early intervention improves cognitive outcomes for preterm infants: randomised controlled trial. Pediatrics. 2010 Nov 1; 126(5): e1088-94.
https://doi.org/10.1542/peds.2010-0778.
[6] Hughes AJ, Redsell SA, Glazebrook C. Motor development interventions for preterm infants: a systematic review and meta-analysis. Pediatrics. 2016 Oct 1; 138(4): e20160147.
https://doi.org/10.1542/peds.2016-0147.
[7] Benzies KM, Magill-Evans JE, Hayden KA, Ballantyne M. Key components of early intervention programs for preterm infants and their parents: a systematic review and meta-analysis. BMC Pregnancy and Childbirth. 2013 Jan 31; 13(Suppl 1): S10.
https://doi.org/10.1186/1471-2393-13-S1-S10.
[8] Puthussery S, Chutiyami M, Tseng PC, Kilby L, Kapadia J. Effectiveness of early intervention programs for parents of preterm infants: a meta-review of systematic reviews. BMC Pediatrics. 2018; 18: 223.
https://doi.org/10.1186/s12887-018-1205-9.
[9] Altunalan T, Sarı Z, Doğan TD, Hacıfazlıoğlu NE, Akman I, Altıntaş T, Uzer S, Akçakaya NH. Early developmental support for preterm infants based on exploratory behaviours: A parallel randomised controlled study. Brain and Behav. 2023 Nov; 13(11): e3266.
https://doi.org/10.1002/brb3.3266.
[10] Birberg Thornberg U, Koch FS, Helmer CS, Tell J, Nyberg E, Abrahamsson T, Mörelius E. Moderate‐To‐Late Preterm Infants Benefit from the Early Collaborative Intervention: Primary Outcomes of an RCT. Acta Paediatrica. 2025 Jun 17.
https://doi.org/10.1111/apa.70173.
[11] Van Hus JW, Jeukens‐Visser M, Koldewijn K, Holman R, Kok JH, Nollet F, Van Wassenaer‐Leemhuis AG. Early intervention leads to long‐term developmental improvements in very preterm infants, especially infants with bronchopulmonary dysplasia. Acta Paediat. 2016 Jul; 105(7): 773-81.
https://doi.org/10.1111/apa.13387.
[12] Silveira RC, Valentini NC, O’Shea TM, Mendes EW, Froes G, Cauduro L, Panceri C, Fuentefria RN, Procianoy RS. Parent-guided developmental intervention for infants with very low birth weight: a randomised clinical trial. JAMA Network Open. 2024 Jul 1; 7(7): e2421896.
https://doi.org/10.1001/jamanetworkopen.2024.21896.
[13] Namprom N, Picheansathian W, Jintrawet U, Chotibang J. The effect of maternal participation in preterm’s care and improved short-term growth and neurodevelopment outcomes. J Neon Nurs. 2018 Aug 1; 24(4): 196-202.
https://doi.org/10.1016/j.jnn.2018.03.003.
[14] Samsudin S, Chui PL, Ahmad Kamar A, Abdullah KL, Yu CW, Mohamed Z. The impact of structured kangaroo care education on premature infants’ weight gain, breastfeeding and length of hospitalisation in Malaysia. J Multidisc Healthca. 2023 Dec 31: 1023-35.
https://doi.org/10.2147/JMDH.S403206.
[15] Maguire CM, Walther FJ, Sprij AJ, Le Cessie S, Wit JM, Veen S, Leiden Developmental Care Project. Effects of individualised developmental care in a randomised trial of preterm infants< 32 weeks. Pediatrics. 2009 Oct 1; 124(4): 1021-30.
https://doi.org/10.1542/peds.2008-1881.
[16] Fan J, Wang J, Zhang X, He R, He S, Yang M, Shen Y, Tao X, Zhou M, Gao X, Hu L. A home-based, post-discharge early intervention program promotes motor development and physical growth in the early preterm infants: a prospective, randomised controlled trial. BMC Paediat. 2021 Apr 7; 21(1): 162.
https://doi.org/10.1186/s12887-021-02627-x.
[17] Kynø NM, Ravn IH, Lindemann R, Fagerland MW, Smeby NA, Torgersen AM. Effect of an early intervention programme on development of moderate and late preterm infants at 36 months: a randomised controlled study. Infant Behav Develop. 2012 Dec 1; 35(4): 916-26.
https://doi.org/10.1016/j.infbeh.2012.09.004.
[18] Lee EJ, Lee SY. The effects of early-stage neurodevelopmental treatment on the growth of premature infants in neonatal intensive care unit. J Exer. Rehab. 2018 Jun 27; 14(3): 523-529.
https://doi.org/10.12965/jer.1836214.107.
[19] Liang X, Miao A, Zhang W, Li M, Xing Y. Effect of family integrated care on physical growth and language development of premature infants: A retrospective study. Transl Pediat. 2022 Jun; 11(6): 965.
https://doi.org/10.21037/tp-22-210.
[20] Smith JR, McGrath J, Brotto M, Inder T. A randomised-controlled trial pilot study examining the neurodevelopmental effects of a 5-week M Technique intervention on very preterm infants. Adv Neon Care. 2014 Jun 1; 14(3): 187-200.
https://doi.org/10.1097/ANC.0000000000000093.
[21] Van Hus JW, Jeukens-Visser M, Koldewijn K, Van Sonderen L, Kok JH, Nollet F, Van Wassenaer-Leemhuis AG. Comparing two motor assessment tools to evaluate neurobehavioral intervention effects in infants with very low birth weight at 1 year. Phys Thera. 2013 Nov 1; 93(11): 1475-83.
https://doi.org/10.2522/ptj.20120460.
[22] Youn YA, Shin SH, Kim EK, Jin HJ, Jung YH, Heo JS, Jeon JH, Park JH, Sung IK. Preventive intervention program on the outcomes of very preterm infants and caregivers: a multicenter randomised controlled trial. Brain Sci. 2021 Apr 29; 11(5): 575.
https://doi.org/10.3390/brainsci11050575.
[23] Yu YT, Hsieh WS, Hsu CH, Lin YJ, Lin CH, Hsieh S, Lu L, Cherng RJ, Chang YJ, Fan PC, Yao NJ. Family-centered care improved neonatal medical and neurobehavioral outcomes in preterm infants: randomised controlled trial. Phys Ther. 2017 Dec; 97(12): 1158-68.
https://doi.org/10.1093/ptj/pzx089.
[24] Gilkison, L. Two approaches for fostering self-regulatory competencies in home-based early childhood education and care: exploring benefits for children’s developing self-regulatory and socio-emotional competencies through the transition to school (Doctoral dissertation, University of Otago).
https://ourarchive.otago.ac.nz/esploro/outputs/graduate/Two-approaches-for-fostering-self-regulatory-competencies/9926478445801891.
[25] Spittle A, Orton J, Anderson PJ, Boyd R, Doyle LW. Early developmental intervention programmes provided post hospital discharge to prevent motor and cognitive impairment in preterm infants. Cochrane Database Syst Rev. 2015(11).
https://doi.org/10.1002/14651858.CD005495.pub4.
[26] Lean RE. Sensitive parenting: a key moderator of neonatal cortical dysmaturation and neurodevelopmental outcomes in children born very preterm. Biol Psyc. 2022 Oct 15; 92(8): 609-11.
https://doi.org/10.1016/j.biopsych.2022.07.010.
[27] Baumann N, Tresilian J, Wolke D. Effects of infant motor problems and treatment with physiotherapy on child outcomes at school-age. Early Human Develop. 2020 Oct 1; 149: 105140.
https://doi.org/10.1016/j.earlhumdev.2020.105140.
[28] Stephenson NL. Child Development for Children Born Too Soon: Identifying Mechanisms and Points for Early Intervention.
https://ucalgary.scholaris.ca/bitstreams/12c8fe24-8f36-4d3e-b043-1523ae63575a/download.
[29] Pirazzoli, L. Affective touch in infancy (Doctoral dissertation, Birkbeck, University of London).
https://eprints.bbk.ac.uk/40410/1/Laura%20Pirazzoli_%20PhD%20thesis_%28includes%20corrections%29.pdf.
[30] Huang X, Chen M, Fu R, He W, He Y, Shentu H, Zhu S. Efficacy of kangaroo mother care combined with neonatal phototherapy in newborns with non-pathological jaundice: A meta-analysis. Front in Paediat. 2023 Jan 25; 11: 1098143.
https://doi.org/10.3389/fped.2023.1098143.
[31] Spratt, A. Teaching Enhanced Milieu Language Skills to Families in Poverty: An Exploratory Study. Minot State University; 2018.
https://search.proquest.com/openview/ee9b6292a7c33bac2b50c084245b3e92/1.pdf?pq-origsite=gscholar&cbl=18750&diss=y.
[32] Pitchik HO, Chung EO, Fernald LC. Cross-cultural research on child development and maternal mental health in low-and middle-income countries. Curr Opin Behav Sci. 2020 Dec 1; 36: 90-7.
https://doi.org/10.1016/j.cobeha.2020.07.013.
[33] Haschke F, Binder C, Huber-Dangl M, Haiden N. Early-life nutrition, growth trajectories, and long-term outcome. In Nestle Nutr Inst Workshop Ser 2019 Mar 13 (Vol. 90, pp. 107-120).
https://doi.org/10.1159/000490299.
Licensed
© 2026 Copyright by the Authors.
Licensed as an open access article using a CC BY 4.0 license.
Article Contents Author Huma Rasheed1, * , Iffat Saeed Channa2 , Samiya Kainat2 , Mohammad Affan Tahir2 1Herbal Biomedicine Inc,
Article Contents Author Murtuza Bhatti 1,2,* Imran Iqbal3 1Bath Spa University, London, United Kingdom; 2BPP University, London, United Kingdom; 3Commecs
Article Contents Author Armaghan Ahmed1, * 1Pediatric Surgery Unit in Social Security Teaching Hospital, Multan, Pakistan Article History: Received: 22
Article Contents Author Aliza Moiz1, * 1Greenwich University, Karachi, Pakistan Article History: Received: 26 November, 2025 Accepted: 24 April,
Article Contents Author Ishaq Kalanther1, * 1Jubail Industrial College, Jubail Industrial City, Jubail, Kingdom of Saudi Arabia Article History: Received:
Article Contents Author Qasem Faisal A Alhajji1, * , Eyad Abdulaziz Abdullah Asiri1, Hassan Majed A Alyousef1, Hamad Jamal Hamad