


Article Contents
Article ID: CMT2621101004
Views: 57Talent Management and Total Quality Management on Patient-Centred Service Quality: Vision 2030 Healthcare Reform as a Moderator
 PDF
PDF
⬇ Downloads: 8
1Imam Abdul Rahman Bin Faisal University, Saudi Arabia
Received: 27 March, 2026
Accepted: 28 May, 2026
Revised: 25 May, 2026
Published: 02 June, 2026
ABSTRACT:
Introduction: This paper examined the associations among Talent Management, Total Quality Management (TQM), and Patient-Centred Service Quality, and explored the moderating effect of Vision 2030 Healthcare Reform in the Saudi Arabian healthcare sector.
Methods: A quantitative research design was employed, with a structured questionnaire using a 5-point Likert scale. Purposive sampling was used to collect data from (n = 350) nurses working in emergency, intensive care, and outpatient units in selected Saudi hospitals. The data was analysed using (PLS-SEM).
Findings: This study revealed that Talent Management Practices and Total Quality Management were statistically significantly related to perceived patient-centred service quality. Perceived patient-centred service quality outcomes were also found to be significantly and positively associated with Perceived Vision 2030 Healthcare Reform. In addition, the moderation results showed that the Perceived Vision 2030 Healthcare Reform initiatives play a significant role in enhancing the relationships among talent management, total quality management, and perceived patient-centred service quality.
Implications: The research highlighted the strategic significance of human capital development, quality management systems, and national healthcare reform efforts in achieving the sustainability of patient-centred excellence. To enhance the sense of institutional accountability and responsiveness to services, policymakers and hospital administrators must incorporate talent strategy and continuous improvement frameworks into the performance requirements of Vision 2030.
Originality Value: This study provided novel empirical evidence by positioning the concept of perceived healthcare reform as a contextual governance mechanism, which allows the study to consider healthcare organisational capabilities as sturdier determinants of perceived healthcare outcomes in the context of patient-centred healthcare reform in Saudi Arabia.
Keywords: Talent management; total quality management; patient-centred service quality; vision 2030; healthcare reform; Saudi Arabia..
1. INTRODUCTION
The The healthcare industry in Saudi Arabia has experienced a significant transformation over the last few years because of a combination of demographic changes, an increase in disease burden, and Vision 2030’s healthcare strategic reforms (Mani & Goniewicz, 2024). (Al-Saggaf et al., 2024; Alharbi et al., 2025) unveiled that service delivery has progressively shifted towards patient-centred care due to substantial developments in the healthcare sector, such as expanding healthcare infrastructure, integrating digital health, implementing privatisation policies, and adopting performance-based governance. (Alasiri & Mohammed, 2022) signifies that enhancing the capacity of healthcare workers along with strengthening quality management systems are important determinants to uphold service delivery, specifically where there are increasing non-communicable diseases with ageing population that lasts to place extra burden on healthcare systems.
Though, following the reforms, Saudi health sector remains with substantial structural challenges. (Rahman & Al-Borie, 2021) claim that the impact of skilled labour shortage, high staff turnover, uneven distribution of skilled labour and quality assurance bottlenecks persist and limit the effectiveness of healthcare services. Besides, due to increasing number of patients and high prevalence of chronic diseases, patient experiences remain unpredictable within healthcare institutions and they have different levels of satisfaction in healthcare institutions (Aljehani & Nawees, 2025). These challenges highlight a gap between policy goals and organisational level of preparedness to achieve consistent patient-centred care outcomes.
The results from the previous studies such as, (Chen et al., 2020; Nkala et al., 2021) show that Talent Management and Total Quality Management (TQM) enhance adaptability of the organisation as well as responsiveness to altering external policies and environmental conditions. For example, (Chen et al., 2020; Nkala et al., 2021) argue that talent strategies for the workforce can improve clinical governance given improved staff competence, staff turnover, and staff adaptability. Likewise, (Salahat et al., 2023) claim that TQM helps to create structured decision making, process standardisation and continuous improvement processes that together bolster the service reliability and patient-centred care delivery.
While there is a massive literature available discussing about different aspects of healthcare transformation such as (Aljehani & Nawees, 2025; Rahman & Al-Borie, 2021) the majority of it has been addressing the subject as three different organisational or policy aspects that are separate from each other, namely Talent Management, Total Quality Management (TQM), and healthcare reforms. There is little empirical evidence that addresses the relationship between these capabilities in Health Care Systems context, especially under the governance conditions imposed by Saudi Vision 2030. Past literature such as (Dzimbiri & Molefi, 2021) is descriptive of the reform attempts, but did not examine the moderating effect of the reform activities on the relationship between organisational capabilities and the patient-centred outcomes. Since then, there has been a lack of focus on the integrated capability frameworks that help describe how the effectiveness of internal organisational capabilities in the delivery of healthcare services is conditioned by institutional reforms.
In terms of theory, a study makes significant contribution towards literature on capability-based models of performance in the field of Resource Based View (RBV) and Total Quality Management (TQM) within healthcare sector of Saudi Arabia. In practice, it provides empirical evidence on the nature of interaction between organisational capabilities, during ongoing healthcare transformation, through the context of Saudi Arabia. In addition, novelty of the study is also its conceptualisation of the process of healthcare reform as a governance-enabling mechanism, thereby not referring to the process of reform as a policy initiative alone, but also as a process that shapes how the capabilities of healthcare organisations come together in a synergistic manner to affect the perceived quality of patients’ services in changing healthcare systems. The study leads to three main contributions: aligning human capital strategies with Vision 2030 healthcare governance reforms.
Support evidence-based quality improvement policies through integrated talent and TQM frameworks.
Test the moderating role of Vision 2030 Healthcare Reform on the relationship between talent management, TQM, and patient-centred service quality using sector-specific data.
2. LITERATURE REVIEW
2.1. Theoretical Framework
The research combines the Resource-Based View and Institutional Theory to explain how organisational capabilities in the healthcare sector can lead to patient-centred service quality, as outlined in the Saudi Vision 2030 healthcare reform. The integrated framework describes the interactions among human capital resources, organisational quality routines, and institutional reform pressures, and their effects on healthcare service outcomes.
As per (Zvarimwa & Zimuto, 2022) the Resource-Based View (RBV) holds that organisations’ performance is reliant on valuable, rare, inimitable, and irreplaceable resources (VRIN). In healthcare organisations, strategic human capital is created through talent management practices such as recruitment, development, and retention, thereby enhancing clinical and service processes. Healthcare talent management boosts professional skills and collaborative proficiencies that contribute to delivering patient-centred care. Similarly, (Kosiol et al., 2023) claimed that specialised healthcare knowledge and skills are inimitable organisational resources that enhance service capacity. Talent management is thus viewed in an RBV perspective as a way of creating a strategic workforce that helps hospitals excel in their services.
Competing theories like institutional theory and the Resource Based View better explain the institutional context for Saudi healthcare transformation under Saudi Vision 2030. For instance, as per (Aldhobaib, 2025) organisational theory of institutions states that organisations respond to external pressures on them in terms of regulatory, normative, cultural pressures which mean that the results of reform for instance, changes in the governance structure, digitalisation and localisation of the workforce, lead to homogenisation of the behaviour of the organisations. In contrast, RBV suggests that institutional pressures have little effect on performance differences because the effects are due to the presence of valuable, rare and inimitable capabilities, which vary from firm to firm suggested by (Kero & Bogale, 2023) also. This forms a boundary condition; policy compliance is not enough to ensure better quality of the services provided if the capabilities within the organisation are not put in place.
However, the assumptions of the Institutional Theory and the Resource-Based View are not completely compatible. (Adubasim et al., 2025; Cha et al., 2024) also suggested that under similar regulatory pressures, organisations evolve towards uniformity regarding structure and practice as hypothesised in Institutional Theory. As per the aforementioned by (Jinjing & Karia, 2024), RBV assumes that performance disparities exist due to different strategic capacities and resource, configuration and positioning among organisations. This presents a theoretical dilemma in the Saudi context due to the need for healthcare to be compliant with the Vision 2030 reforms, but not necessarily achieve better patient-centred outcomes. The governance structures that can be adopted to reform a hospital can be in place at the formal level, but there are variations in staff competence, managerial readiness, and systems of quality in hospital operations. Thus, it is important to combine and take both views into account to bring out reasons for variation in the ability of some healthcare organisations to implement the change in services in response to reform pressures.
2.2. Hypotheses Development
2.2.1. Talent Management and Perceived Patient-Centred Service Quality
Empirical literature has evidenced that talent management is a strategic factor in service quality in healthcare systems. In this perspective, (Irtaimeh et al., 2016) also investigated this relationship based on the survey data concerning the Jordanian healthcare industry and 135 valid responses at the Princess Rahma Hospital reported the statistically significant positive effect (P < 0.05) of the strategies of talent management in improving the quality of the provided service and satisfaction of beneficiaries. Although their study’s results helped explain the performance-enhancing nature of talent strategies, the cross-sectional design and single-hospital setting limit generalisability and causal inference. (Aljehani & Nawees, 2025; Friedel et al., 2023; Nilsen et al., 2020) also address the role of service differentiation as a result of human capital capabilities within the Resource-Based View. Nevertheless, moderating processes and longitudinal impacts were not tested in the research. The review (2019-2024) suggests that nursing talent management, with a focus on leadership development, digitalisation, and mentoring, contributes to better patient care quality and the sustainability of the workforce. The review-based design is considered comprehensive but lacks primary empirical validation and may be prone to selection bias. Contrarily, (Alharbi et al., 2025; and Salahat et al., 2023) argue that strategic talent pools have a direct effect on service innovation, consistent with the RBV claim that rare competencies are performance drivers. However, they have much work that is conceptual and non-healthcare-based.
Other empirical evidence has complementary information. For instance, (Pereira et al., 2023; and Al-Saggaf et al., 2024) concluded that talent retention significantly enhanced hospital service responsiveness in Gulf environments, although the measurements were based on perceptual scales. Relating the findings to Total Quality Management, competence of employees is the key to the ongoing improvement process, as suggested by (Rave et al., 2022; and Alasiri & Mohammed, 2022), while also emphasising regularly organised workforce participation in quality systems. Nevertheless, integrating talent management into quality frameworks is not a common practice in most healthcare studies, which treat it as an HR activity. The combined arguments help confirm a positive relationship between talent management and service outcomes, but demonstrate a lack of integrated, theory-driven empirical research in Saudi Arabia.
Further, previous research comprising (Chen et al., 2020; Nkala et al., 2021). indicates that talent management positively impacts healthcare performance by boosting the capability of employees, engagement and responsiveness in delivering services to patient. Nevertheless, there is contradictory evidence provided by (Rahman & Al-Borie, 2021) regarding the strength and significance of the link in some healthcare environments as staffing is poorly managed, human resource practices are poorly designed to fit into operational systems, and there is limited retention device. Thus, organisational preparedness, stability of staff, backing of the leadership and the extent of integration of HR practices within healthcare systems are among the factors that impact the effectiveness of talent management. In the context of the healthcare sector in Saudi Arabia, these discrepancies are also driven by the Saudi Vision 2030 implementation, which is still in its early stages, with its transformative efforts ever progressing towards the introduction of rapid reforms, localisation of Saudi workforce and digitalisation. There are conflicting views in the current work around positive outcomes obtained from talent management in health care environments. In the context of a Resource Based View, Talent Management is about building rare and valuable human capital competencies that impact the organisation’s performance. Though, from an institutional and process perspective, the approach of talent strategies alone is not adequate to enhance service results without the help of operational integration, leadership buy-in and quality governance systems. These two views imply that the ties between talent management and an experience of service quality in the patient’s perspective is not necessarily uniform for all healthcare systems. Thus, based on these perspectives, H1 of the study is formulated;
H1: Talent Management possess statistically significant relationship with Perceived Patient-Centred Service Quality in the healthcare sector of Saudi Arabia.
2.2.2. Total Quality Management and Perceived Patient-Centred Service Quality
(Haroun et al., 2022; Rahman & Al-Borie, 2021) define TQM as a multidimensional philosophy encompassing customer focus, employee involvement, and continuous improvement, and argue that all three dimensions can improve patient experiences and outcomes. Their findings are quite consistent with the classical theory of TQM, which assumes that a systemic quality culture spurs excellence in service. Nevertheless, their narrative assessment is largely quantitative, which limits empirical accuracy and does not provide empirical evidence that TQM has a direct effect on perceived service quality and patient satisfaction, and that satisfaction moderates’ behavioural intentions. Even though their structural modelling enhances causal inference, they are based on perceptual survey data, which invokes the issue of common method variance and inflated correlations. Likewise, (Zafar et al., 2025) indicate that patient care and service quality have improved following TQM implementation, which supports the argument that continuous improvement is at the core of TQM theory. On the other hand, (Almutairi et al., 2024; Essa, 2025) indicate that barriers to implementation in Saudi public hospitals include poor organisational culture and moderate levels of workforce satisfaction, suggesting that TQM’s effectiveness is context-dependent and not universal. This is partly contrary to the more positive results of (Zaid et al., 2020), who noted that there is diversity in the institutional contexts. (Shehadeh & Bin Ahmad, 2025) also make it more complicated as they show that strategic management is a moderating factor in the TQM-service quality relation, which means that TQM itself, without strategic alignment, can be ineffective.
The prevailing theme in studies is that leadership commitment and workforce empowerment are quality enablers, but there are conflicting arguments over whether TQM has a direct impact or operates through moderators. Most studies use a cross-sectional survey design, which does not allow longitudinal insight or objective measurement of outcomes. A theoretical perspective on TQM is that of continuous quality improvement, but through the prism of the Resource-Based View, quality systems are seen as strategic capabilities that need to be integrated into the organisational context.
The overall evidence is generally positive but there is not consistent evidence available regarding the relationship between Total Quality Management (TQM) and the service quality perceived by patients. Previous studies such as (Grossu-Leibovica & Kalkis, 2023; Tessema et al., 2024) indicated that TQM can be used to enhance the performance of the healthcare sector by implementing continuous improvement, actively involving employees, leading with continuous commitment by the leaders, and optimising processes, which in turn would improve the quality of services provided to the patients. Though, counterintuitive results provided by (Atalıç & Çiçek, 2021; Zafar et al., 2025) suggests that TQM can be superficial, have limited support from leadership or organisational readiness and have weak and/or insignificant effects. This suggests that the impact of TQM is strongly dependent on organisational culture, leadership commitment, and employee participation and readiness of the institution, especially in the health sector where there is a swift changing landscape. However, in Saudi Arabia, inconsistent factors are also affected by the continuous healthcare transformation that is taking place in the Kingdom under the Saudi Vision 2030, including digitalisation of hospitals, governance reform and restructuring of the healthcare workforce. There are also conflicting views on the success of TQM in healthcare systems in the literature. As per (Pereira et al., 2023) the traditional theory of TQM suggests that service quality outcomes are generally improved through the introduction of standardisation, a continuous improvement approach and through participation of the workforce. The other views that are mainly contingency-oriented claim that the success of TQM is highly contingent on cultural aspects, managerial competencies, institutional readiness and employee motivation. Formal quality routines can be in place and symbolic, that is not routinely used in clinical practice in rapidly changing health care systems. As a result, TQM and the perceived patient-centred service quality can be seen as being very different in different institutional and governance settings. Hence, there is a gap in the empirical evidence, as there is no strong, Saudi-specific, theory-based relationship testing. Based on emerging arguments from the above literature, the following hypothesis (H2) is developed.
H2: Total Quality Management shows a statistically significant association with Perceived Patient-Centred Service Quality within the healthcare sector of Saudi Arabia.
2.2.3. Moderating Effect of Perceived Vision 2030 Healthcare Reform
The transformation in healthcare under the Perceived Saudi Vision 2030 has been a broadly researched structural reform agenda that is projected to boost efficiency, accountability, privatisation, digitalisation, and workforce development in the national health system, as suggested by (Akdere et al., 2020). (Alharbi, 2021; Alfahad et al., 2024) indicates that the restructuring of governance through reforms strengthens the ability of an institution to operate through indirect impacts on the quality of services delivered. In similar vein, (Rahman & Al-Borie, 2021) state that digital health programmes and e-governance systems led to the improvement of accessibility and responsiveness of services, but such studies are cross-sectional, which limits the ability to infer over time.
In comparison, (Alanezy et al., 2025; Dzimbiri & Molefi, 2021) show that policies of workforce localisation and competency development contributed to higher employee engagement and commitment to the organisation, suggesting that the reform initiatives strengthen the alignment of human capital. Although these results align with the Resource-Based View, which postulates that the institutional framework enhances the value extraction of strategic resources, the methodological rigour of the studies differs. The majority of them depend on the perceptual survey tools or case-based assessment and do not allow objective analysis of patient-centred service outcomes, which is indicated in the findings of (Pereira et al., 2023; Salahat et al., 2023) as well.
Total Quality Management is considered to adopt institutional changes for continuous improvement, including governance changes, performance measurement systems, integration among departments, and electronic monitoring systems, according to evidence highlighted by (Al-Arabiya, 2023; Graham et al., 2024) also. These processes build quality–performance linkages, by incorporating structured operational practices into healthcare organisations. In contrast, existing empirical research such as (Aljehani & Nawees, 2025; Ali & Dzandu, 2023) however, generally focuses on the relationships between talent management, TQM or healthcare reform separately without putting them in a single structure. This raises the conceptual ambiguity of how the implementation of reform policies in healthcare organisations contribute to the strengthening of their capacities or its efficacy depends on their readiness, managerial capacities. This can generate conceptual confusion on the effect that reform policies have when they lead to the strengthening of the capacity of the organisations or whether their effectiveness depends on institutional readiness, capabilities of managers, and the operational implementation of reform policies in the organisations themselves. Additionally, there is a lack of a clear structural conditioning mechanism in the perceived Vision 2030 healthcare reform, leaving the understanding of the impact of institutional reforms on the relationship between the capacities of the healthcare organisations and the quality of services provided to be limited, therefore a moderation-based analysis is needed in the Saudi healthcare context. These emerging arguments from the literature, following H3 of the study is developed. On the other hand, the identification of gaps in existing body of knowledge and the formulated research objectives, following conceptual framework of the study is illustrated in Fig. (1).
H3: Perceived Vision 2030 Healthcare Reform statistically and significantly moderates the relationship of Talent Management and Total Quality Management with Perceived Patient-Centred Service Quality in the Saudi Arabian context.
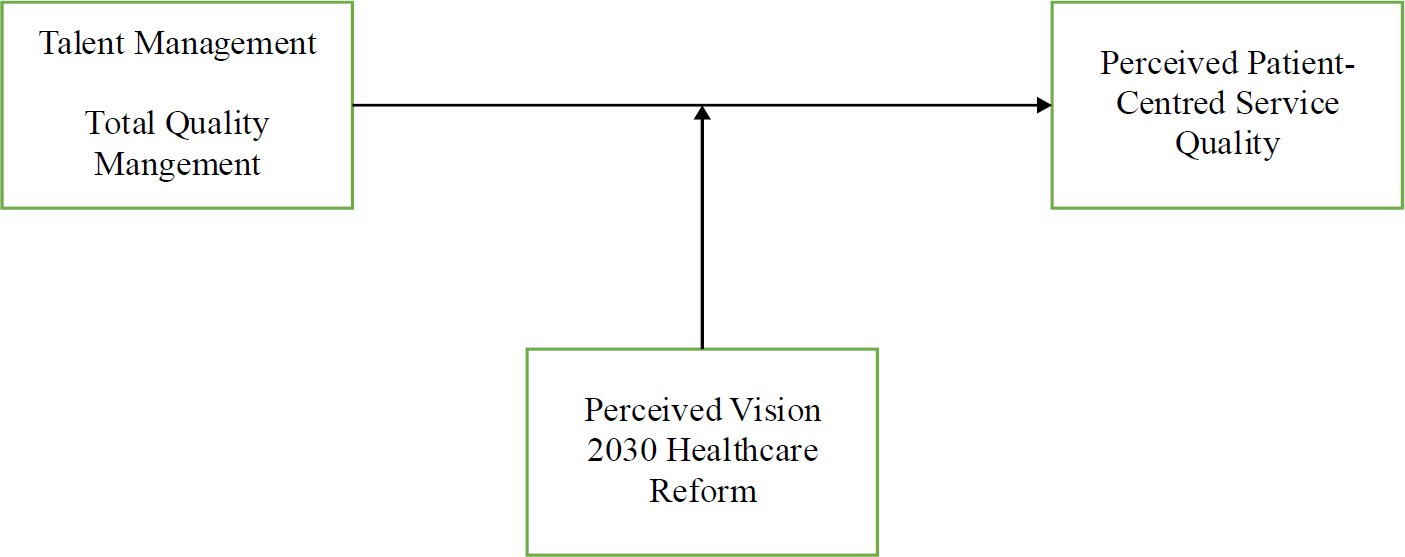
Fig. (1). Conceptual framework.
3. METHODS
In this study, a primary quantitative research design is employed, with data collected via a structured Likert-scale questionnaire. Terms were rated on a five-point scale, with 1 (strongly disagree) as the lowest and 5 (strongly agree) as the highest, as suggested by (Tanujaya et al., 2022). The instrument was segmented into four constructs, including Talent Management, Total Quality Management, Perceived Patient-Centred Service Quality, and Perceived Vision 2030 Healthcare Reform, as depicted in the Appendix A.
3.1. Population
The study population included the registered nurses in public and private hospitals in Saudi Arabia. The Saudi Commission for Health Specialties reported that the number of nurses working in Saudi Arabia is more than 230,000, working in various hospitals and health facilities. Nurses in emergency, intensive and outpatient services were selected because they come into direct contact with service delivery of the patient and have direct operational experience of healthcare reform and quality systems in hospitals, and they are specially selected for their role in the hospital’s patient service.
3.2. Sample Size
To the target population, 350 nurses were selected using purposive sampling technique. As it allows to select the respondents with specific knowledge and experience relevant to the study’s variables. Since the proposed study aims to consider reform implementation and quality practices, purposive sampling was used to ensure the inclusion of participants who are actively involved in patient care processes, as used by (Obilor, 2023; and Tajik et al., 2025) in their studies. The G*Power formula for calculating sample size when multiple regression is used was used: N = (Za + Zb)2 x (1 – R2)) / R2. The lowest possible sample size was 129, assuming an effect size (f2 = 0.15), a power of 0.95, and four predictors. Nonetheless, 600 questionnaires were distributed to increase statistical power and external validity. The response rate was 63.3% with 380 returned questionnaires. Though, 30 questionnaires were eliminated due to missing values and multivariate outliers identified by the Mahalanobis distance resulting in a final sample of 350.
Even though respondents were from various hospitals, the current study collected data at the individual level, as the primary objective was to assess individual perceptions of talent management, total quality management, and reform implementation, rather than to compare hospital-level performance. This study is therefore not within the capabilities of aggregating the data at the organisational level. Therefore, future studies could consider applying multilevel modelling to account for cross-level effects and address hospital-level variation in the implementation of the reform and in quality outcomes.
3.3. Addressing Bias
Selection bias was reduced as the respondents were selected to represent various hospital units and both public and private sectors. As recommended by (AboAlsamh, 2025), the risk of non-response bias was addressed by conducting an independent-samples t-test on the early (n1 = 30) and late respondents (n2 = 30), and all results were found to be statistically equal. Common method bias (CMB) was treated both statistically procedurally. Anonymity was guaranteed as items were well randomised in the questionnaire and clear instructions were used to minimise social desirability and evaluation apprehension effects. Both Harman’s single-factor test and the full collinearity assessment indicated that variance explained by a single factor was below 50% as suggested by (Howard et al., 2024) also. The integrated methods suggest that the resulting relationships observed in the model are unlikely to be significantly distorted by CMB.
3.4. Ethical Considerations
This study obtained ethical approval from the university’s Institutional Research Ethics Committee before data collection. The research adhered to the internationally recognised research ethics when dealing with human subjects. The administration officials of the involved hospitals also granted the researcher the right to administer the survey questionnaires. Respondent participation was voluntary, and informed consent was obtained from all participants. The questionnaire included an effective statement of the research aim, confidentiality, and the right to withdraw from the research at any time without repercussions. The collection of personal identifiers was not carried out, and the anonymity and confidentiality of the respondents’ professional and personal information were maintained throughout the research process.
Data Analysis
The data were analysed using Partial Least Squares Structural Equation Modelling (PLS-SEM). Reliability was evaluated using measurement model assessment with Cronbach’s alpha and composite reliability, and convergent validity was assessed using Average Variance Extracted (AVE) as suggested by others. This was followed by testing hypothesised causal and moderating relationships through path analysis in PLS-SEM. The study was conducted with a prediction-oriented purpose and the requirement of examining direct relations among constructs in combination with the moderating relations among these constructs also led to the selection of PLS-SEM. While the sample size (n = 350) is adequate for CB-SEM, the covariance-based techniques are more suitable to confirm a theory and to analyse the stringent model fits within the multivariate normality assumption. Compared to this, PLS-SEM is suggested for the models with a number of predictive steps and variance maximisation particularly when it has moderation effects, as mentioned by (Dash & Paul, 2021). It is also robust in the presence of data distributions other than normal. Besides, PLS-SEM is less dependent on non-normality and is appropriate for an exploratory integration of various theoretical approaches in intricate moderation frameworks (Al Issa & Abdelsalam, 2021). Hence, PLS-SEM is more suitable in estimating direct and moderating effects in the proposed framework.
4. RESULTS
4.1. Demographics Analysis
Table 1 shows the demographic profile of the study participants from the total sample (n = 350). The statistics show that, across the total sample, 45.71% were male, 50% were female, and 4.29% preferred not to say. Among these participants, 18.57% were under 25 years old, 21.43% were 25-34 years old, 24.29% were 35-44 years old, 17.14% were 45-54 years old, and 18.57% were 55 years old or older. Furthermore, in the total sample, the largest proportion of participants held Bachelor’s degrees (31.43%), followed closely by Master’s degrees (30%). Moreover, with regard to the current job role, 42.86% of the nurses serve as Operational/Frontline workers, 35.71% serve in supervisory positions, and only 5.71% serve in senior management roles. Also, with regards to industry experience, most participants held 6–10 years (36.86%) and more than 10 years (28.86%) of experience. Also, among total participants, 38.57% worked in public government hospitals, 32.86% in private hospitals, and 28.57% in military specialised hospitals. Lastly, regarding regional context, 31.43% and 38.57% of the total population are served by hospitals in the central and western regions of Saudi Arabia, respectively.
Table 1. Demographics profile analysis.
| Demographic Category | Frequency (n) | Percentage (%) | |
| Gender | Male | 160 | 45.71% |
| Female | 175 | 50.00% | |
| Prefer not to say | 15 | 4.29% | |
| Age Range | Below 25 | 65 | 18.57% |
| 25–34 | 75 | 21.43% | |
| 35–44 | 85 | 24.29% | |
| 45–54 | 60 | 17.14% | |
| 55 and above | 65 | 18.57% | |
| Educational Qualification | Secondary | 60 | 17.14% |
| Diploma | 75 | 21.43% | |
| Bachelor’s | 110 | 31.43% | |
| Master’s | 105 | 30.00% | |
| Current Job Role | Operational/Frontline | 150 | 42.86% |
| Supervisory | 125 | 35.71% | |
| Managerial | 55 | 15.71% | |
| Senior Management | 20 | 5.71% | |
| Industry Experience | Less than 3 years | 55 | 15.71% |
| 3–5 years | 65 | 18.57% | |
| 6–10 years | 129 | 36.86% | |
| More than 10 years | 101 | 28.86% | |
| Hospital Type | Public government hospital | 135 | 38.57% |
| Private hospital | 115 | 32.86% | |
| Military / Specialised government hospital | 100 | 28.57% | |
| Geographic Region | Central | 110 | 31.43% |
| Eastern | 135 | 38.57% | |
| Western | 105 | 30.00% | |
4.2. Measurement Model Assessment
The measurement model of the study is tested for internal consistency reliability and convergent validity using approaches that include Cronbach’s Alpha, Composite Reliability with threshold values of 0.7, and Average Variance Extracted (AVE) with a threshold value of 0.5, as suggested by (Baharum et al., 2023; Baistaman, 2020) also.
The results of the measurement model assessment as shown in Table 2, indicate high factor loadings, ranging from 0.639 to 0.929. Further, the results also depict that the internal consistency and reliability have been attained since Cronbach’s Alpha and Composite Reliability values in the case of all constructs of the study are found to be (α > 0.7). Lastly, convergent validity is established, as the AVEs exceed the threshold of 0.5. The measurement model of the study is signified in Fig. (2).
Table 2. Measurement model assessment.
| Latent Variables | Indicators | Factor Loadings | Cronbach’s Alpha | Composite Reliability | Average Variance Extracted |
| Perceived Patient-Centred Service Quality | PCSQ1 | 0.914 | 0.902 | 0.905 | 0.837 |
| PCSQ2 | 0.929 | ||||
| PCSQ3 | 0.901 | ||||
| Talent Management | TMP1 | 0.877 | 0.840 | 0.843 | 0.758 |
| TMP2 | 0.892 | ||||
| TMP3 | 0.841 | ||||
| Total Quality Management | TQM1 | 0.826 | 0.832 | 0.845 | 0.749 |
| TQM2 | 0.914 | ||||
| TQM3 | 0.855 | ||||
| Perceived Vision 2030 Healthcare Reform | V2HR1 | 0.639 | 0.896 | 0.896 | 0.592 |
| V2HR2 | 0.743 | ||||
| V2HR3 | 0.750 | ||||
| V2HR4 | 0.908 | ||||
| V2HR5 | 0.763 | ||||
| V2HR6 | 0.788 |
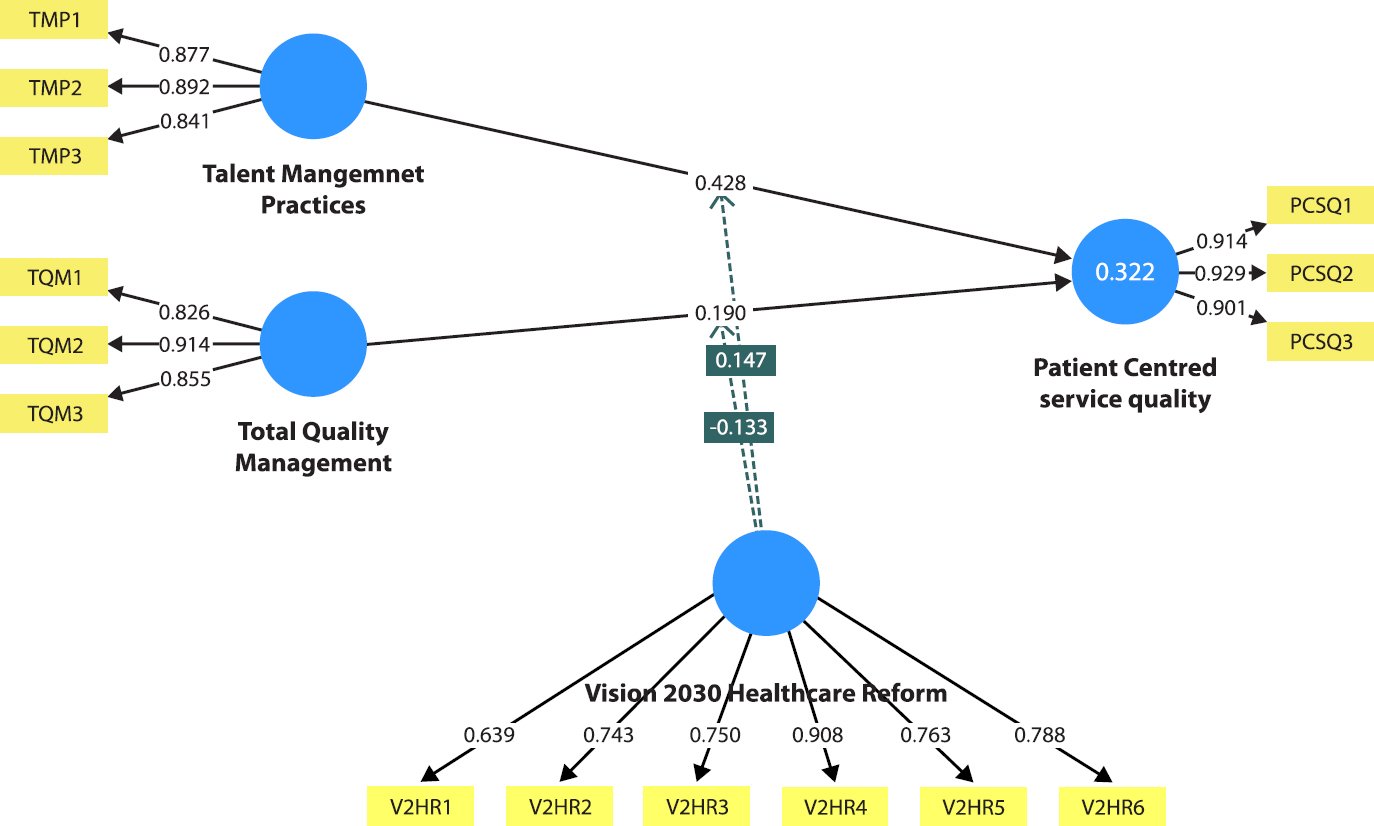
Fig. (2). Measurement model of the study.
4.3. Discriminant Validity
The discriminant validity, which examines the conceptual overlap and distinctiveness among the model’s constructs, is assessed using the HTMT ratio, with a threshold of 0.85, as indicated by (Rasoolimanesh, 2022).
The results in Table 3 show that all inter-construct HTMT ratios are below the threshold, indicating sufficient discriminant validity. In particular, Talent Management Practices reported low HTMT values with Perceived Patient-Centred Service Quality (0.612) and Total Quality Management (0.602), indicating that there is no conceptual overlap or separability between the constructs. Similarly, Total Quality Management also shows a low HTMT value with Perceived Patient-Centred Service Quality (0.453), indicating separability among these constructs. The conceptual distinctiveness of Perceived Vision 2030 Healthcare Reform is also supported by low HTMT values for all constructs (0.069-0.128). Generally, the results show that construct separability is achieved with no conceptual overlapping.
Table 3. Discriminant validity.
| – | Perceived Patient-Centred Service Quality | Talent Management Practices | Total Quality Management |
| Talent Management Practices | 0.612 | – | – |
| Total Quality Management | 0.453 | 0.602 | – |
| Perceived Vision 2030 Healthcare Reform | 0.069 | 0.128 | 0.124 |
4.4. Variance Inflation Factor
The variance inflation factor (VIF) allows for assessing multicollinearity and addressing the issue of common method bias (CMB). The threshold value of VIF is generally ≤ 3.5.
The VIF results, as shown in Table 4, indicate values within the acceptable limit of ≤ 3.5, suggesting no issues of multicollinearity or common method bias.
Table 4. Variance inflation factor.
| – | VIF |
| Talent Management Practices -> Perceived Patient-Centred Service Quality | 1.811 |
| Talent Management Practices -> Perceived Vision 2030 Healthcare Reform | 1.347 |
| Total Quality Management -> Perceived Patient-Centred Service Quality | 1.405 |
| Total Quality Management ->Perceived Vision 2030 Healthcare Reform | 1.347 |
| Perceived Vision 2030 Healthcare Reform -> Perceived Patient-Centred Service Quality | 1.691 |
4.5. Path Coefficient Analysis
The results of the path coefficients, shown in Table 5, indicate that both organisational capability variables have statistically significant relations with perceived patient-centred service quality. The results in Table 5 indicate that the Talent Management Practices have a positive relationship with perceived patient-centred service quality (β = 0.428, p < 0.000). In a similar manner, Total Quality Management demonstrates a statistically significant, positive association with the perceived patient-centred quality of service (β = 0.190, p < 0.003). Moreover, Perceived Vision 2030 Healthcare Reform has a positive, statistically significant relationship with perceived patient-centred service quality (β = 0.141, p < 0.041), indicating that healthcare personnel who perceive reform initiatives as effectively implemented would report greater perceived patient-centred service delivery.
Table 5. Path coefficient.
| – | Path coefficients | T-statistics | P-values | F-square |
| Talent Management Practices -> Patient-centred service quality | 0.428 | 7.148 | 0.000 | 0.195 |
| Total Quality Management -> Patient-centred service quality | 0.190 | 2.937 | 0.003 | 0.037 |
| Vision 2030 Healthcare Reform -> Patient-centred service quality | 0.141 | 2.051 | 0.041 | 0.002 |
| Vision 2030 Healthcare Reform x Talent Management Practices -> Patient-centred service quality | 0.147 | 2.119 | 0.022 | 0.018 |
| Vision 2030 Healthcare Reform x Total Quality Management -> Patient-centred service quality | 0.133 | 2.825 | 0.003 | 0.013 |
Note: *: Significance at 10%; **: Significance at 5%; ***: Significance at 1%
The moderating analysis also demonstrates that Perceived Vision 2030 Healthcare Reform moderates the association between organisational capabilities and the perceived service outcomes. Also, the relationship between Perceived Vision 2030 Healthcare Reform and Talent Management Practices is positive and statistically significant (β = 0.147, p < 0.022), indicating that stronger perceptions of the reform’s implementation strengthen the association between talent management and perceived patient-centred service quality. Similarly, the association between Perceived Vision 2030 Healthcare Reform and Total Quality Management is statistically significant and positive (β = 0.133, p < 0.003), indicating that the reform-based institutional support enhances the value of quality management practices for patient-centred service quality. Lastly, in terms of effect size, the results of the F-square shows different effect sizes of predictors when predicting Patient-Centred Service Quality. Talent Management depicts a moderate effect (f² = 0.195), which signifies moderate effect size. Total Quality Management also shows a small effect (f² = 0.037), whereas perceived Vision 2030 reform depicted negligible effect size (f² = 0.002). Interaction effects are also small but pertinent, which validates limited, though, meaningful moderating effect in the structural model.
From a practical perspective, talent management, with its higher effect size, has the large influence on the perception of the quality of service provided in the healthcare sector in Saudi Arabia, in comparison with procedural quality systems. This indicates that there is a need for hospital management to emphasise leadership development, digital competency training, strategies for retaining staff and strategies to engage their workforces to boost their responsiveness to services. The interaction of TQM and reform are relatively weak but are statistically significant, showing that there is still a reinforcement between structured governance and reform-enabling institutional settings and organisational performance. Hence, aligning quality monitoring systems and workforce strategies to Vision 2030 performance indicators with the aim of maximising healthcare outcomes from the patient perspective is a critical priority of healthcare managers.
4.6. Model Explanatory Power
The results shown in Table 6 specify moderate explanatory power of the measurement model. It can be observed that 32.2% of the variation in Perceived Patient-centred service quality can be predicted by TQM, talent management practices, and perceived Vision 2030 health reforms.
Table 6. Model explanatory power.
| – | R-Square | R-Square Adjusted |
| Perceived Patient-Centred Service Quality | 0.322 | 0.312 |
4.7. Q-squared
As shown in Table 7, the Q²predict value for perceived patient-centred service quality is 0.296, which is greater than zero, indicating that the model has sufficient predictive relevance. Also, the RMSE (0.850) and MAE (0.627) values indicate satisfactory prediction accuracy, which supports the structural model’s out-of-sample predictive capability for the dependent construct.
Table 7. Q-squared-predictive relevance.
| – | Q²predict | RMSE | MAE |
| Perceived Patient-Centred Service Quality | 0.296 | 0.850 | 0.627 |
5. DISCUSSION
The results validate H1, as Talent Management Practices show a statistically significant relationship with Perceived Patient-Centred Service Quality in Saudi healthcare. This aligns with (Irtaimeh et al., 2016), who found a strong positive relationship between talent strategies and service quality in Jordan. Similarly, (Mat, 2025) highlighted the use of leadership, mentorship, and digital competencies in nursing as essential processes of improving the quality of patient care. Nevertheless, compared with (Rahman & Al-Borie, 2021), who implied that HR practices must be moderated by other factors, including employee engagement, to shape service outcomes, current research shows a direct association in Saudi Arabia.
This disparity can be justified by centralised healthcare governance and systematic workforce changes in Saudi Arabia as part of Vision 2030, which better incorporate talent development into hospital performance outcomes (Rahman & Al-Borie, 2021). Comparatively centralised administrative structures characterising healthcare institutions of Saudi Arabia may be connected to robust compliance to competency frameworks across organisational settings which leads to higher visibility of talent management activities in patient-centred practices disclosed by (Essa, 2025) also. The strategic value of skilled healthcare professionals could be further enhanced in the industrial sector due to rapid digital transformation and nationalisation of workforce (Saudisation) policies. From the viewpoint of Resource-Based View, (Alharbi et al., 2025) also highlights that human capital signifies a strategic organisational resource and its efficient usage leads to improved service delivery in healthcare organisations. Talent management aligns institutional capabilities with patient expectations, thereby improving its applicability in Saudi healthcare settings.
The increasing digitisation of healthcare services in Saudi Arabia, including smart hospital management, predictive analytics, digital engagement platforms for patients, and AI-driven data-driven quality monitoring further underscores the importance of digitally knowledgeable healthcare practitioners who can thrive in technologically advanced healthcare settings. (Kosiol et al., 2023) claim that such skills involve tacit knowledge that is difficult to be copied and that requires both clinical expertise and digital competence in the healthcare sector. Though, (Atalıç & Çiçek, 2021) propose that an ability to work in a team and in a patient-centred manner is made institutional over time in the process of talent development in the health sector. In Vision 2030, the critical role of digitally competent healthcare workers is growing due to growing digital health systems and electronic governance highlighted by (Alfahad et al., 2024) also. As a result, talent management builds valuable and scarce human capital assets that enhances organisational flexibility and enables a focus on delivering patient-centred services.
The findings suggest that Total Quality Management (TQM) and Perceived Patient-Centred Service Quality are significantly associated, thereby justifying the acceptance of H2. This result supports (Zaid et al., 2020), who found that TQM has a significant impact on patients’ perceived service quality and satisfaction in Palestinian healthcare organisations. The conceptual focus of (Haroun et al., 2022) is that customer focus, continuous improvement, and integrated systems improve patients’ experiences, and current study empirically tests these arguments in Saudi hospitals. In current study, TQM signifies organisational process capability, while patient-centred service quality imitates perceived service outcomes confronted by patients across healthcare delivery settings.
Application of TQM in Saudi public healthcare organisations may confront limitations related with relatively low levels of job satisfaction as well as developing organisational culture conditions, as informed by (Almutairi et al., 2024). Other such as (Alanezy et al., 2025) argue that these restrictions could be an outcome of transitional resistance to organisational restructuring, reform fatigue, pressure on the workforce when adapting to change and managerial readiness, which may arise as part of the process of implementing the reforms in Vision 2030, as posited by (Alanezy et al., 2025). Therefore, the impact of TQM can be different depending on the level of adaption, employees’ attitudes towards the organisation and institutional supports provided throughout the health care organisations. However, (Ali & Dzandu, 2023) suggests that observed relationship between TQM and perceived patient-centred service quality is also influenced by the growing “pressure” on the organisation for pursuing standardised quality indicators and accreditation processes, not just by the maturity of the organisation itself.
These findings are theoretically extended to organisational capability theory, as these phenomena are not only institutional pressures that come from the outside of the organisation, but are part of the context from which the organisational capability produces service outcomes. In this context, TQM is considered to be not only an operational quality system but also a capability for governance, which is supported by a digital monitoring system and through the generation of accountability mechanisms and performance appraisal which was also mentioned by (Al-Saggaf et al., 2024) as a governance-driven performance evaluation system. This contradicts the conventional RBV assumption of the independence of the capabilities from the institutional setting. However, the study reveals that the organisational capacity is enhanced when it merges with reform-oriented governance mechanisms. The study thus helps to develop a new paradigm that sees as essential that the effectiveness of capabilities within health institutions is dependent on the context in which they are situated rather than generalisable.
The moderating analysis that supports H3 shows that Perceived Vision 2030 healthcare reform has a significant positive moderating effect on the relationship between organisational capabilities and the perceived quality of patient-centred services. In particular, the interaction effects of perceived Vision 2030 reform and both Talent Management and Total Quality Management are positive, suggesting that reform initiatives improve the degree to which they said internal capabilities are converted to the enhanced image of service delivery at the patient level, as revealed in the findings of (Nilsen et al., 2020) as well.
If hospitals see Vision 2030 reform as stronger and beneficial in terms of driving operational excellence of the healthcare organisations, they can place more emphasis on performance monitoring systems, digital governance systems, accreditation systems and outcome-based managerial evaluations as a way to add organisation accountability. Structures of governance designed for reform can enhance the operationalisation of TQM routines and talent management processes through improved compliance, intra-departmental coordination and data-driven decision making which is suggested by (Haroun et al., 2022) also. As a result, healthcare professionals feel more aligned with the goals of patient-centred care, which can enhance the impact of quality management and staff skills on patient outcomes in Saudi healthcare facilities.
The results are also applicable to the international healthcare setting. In line with (Rahman & Al-Borie, 2021), the similar reform-oriented healthcare modernisation programmes have been noted in the NHS’s digital transformation in the United Kingdom as well as the Asian healthcare systems which focus on smart governance, performance-based accountability and integration service delivery models. Though, whereas more decentralised reform settings found in (Graham et al., 2024) lack of strong central coordination and governance of the workforce, the Saudi healthcare transformation offers greater level of central governance coordination via Vision 2030, which may allow for more direct coupling between the capability of the workforce, quality systems, and institutional reform agendas. This means that the performance of the organisational capabilities might vary strongly by national governance arrangements, the state of healthcare reforms and the capacity of institutions to implement them.
There is a competing explanation that centralisation led to unequal results based on the level of autonomy granted in the organisations and their capacity to implement the policies and performance systems, as proposed by (Pereira et al., 2023) also. Therefore, centralisation does not necessarily result in better performance, but rather works in conjunction with institutional readiness and managerial skills. Theoretically, these results offer a way to advance the institutional logic to demonstrate that reforms work as contingent mechanisms, or are not necessarily enabling structures; they go beyond the merely confirmatory way of understanding the effectiveness of reform.
Although the evidence for health reforms has been ‘moderating’, it is important to note that this does not necessarily mean that such reforms will be carried out equally across all hospitals. In some healthcare environments, quality management systems and employee initiatives are less effective due to reform fatigue, symbolic compliance with accreditation standards, bureaucratic overload, implementation capacity issues and resistance to digital transformation. Excessive administrative oversight can also distract focus from interacting with the patient and focus more on compliance. Therefore, the effectiveness of reforms under Vision 2030 is contingent on the readiness of the institutions, managerial adaptability, acceptance of the workforce, and capacity to integrate the technology into the healthcare organisation, and as such cannot be considered as universally enabling mechanisms.
Healthcare organisations have been symbolically implementing reform-oriented quality systems for the purposes of compliance deprived of completely integrating them into operational practice. Institutional decoupling can occur when there is a gap between governance and performance, in the sense that the formal accreditation framework exists, but the corresponding performance is inadequate to ensure patients’ outcomes are centred. Likewise, the hospitals with heavy workloads tends to focus more on the formality of the work than on realising meaningful service innovations. The effectiveness of reform-governance therefore, rely on the level of operational self-integration of quality systems into daily clinic and managerial processes.
According to the theory of Resource-Based View, perceived Vision 2030 reform improves the strategic utilisation of organisational valuable resources, especially human capital, which is nurtured through talent management practices (Pereira et al., 2023). At the same time, according to Total Quality Management theory, the institutionalisation of continuous improvement routines and performance monitoring in healthcare organisations is attained by reform-driven mechanisms of governance (Cha et al., 2024). The moderating findings thus indicate that reform is their institutional facilitator, reinforcing the performance of organisational capabilities rather than substituting for them. Therefore, the result shows that the integration of governance mechanisms, capability building development of healthcare workers, systems of a digital transformation and quality management routines become strategically effective to healthcare reforms. This strengthens the policy orientation of the need for regulatory change, as well as for readiness of institutions, adaptability of management, and support of technologically mediated governance infrastructures for long-term healthcare performance in favour of patients.
Potential differences between the various healthcare organisations, such as public versus private and military, also shape the perception and implementation of the changes in the hospitals towards the implementation of Vision 2030. Aas highlighted by (Zafar et al., 2025) also, the public hospital in Saudi Arabia perceive reform more as administrative restructuring, finding localised staffing arrangements, or accountability measures, while private hospitals feel reform more as market competitiveness or privatisation pressure, and efficiency expectations. Likewise, there can be individual operational autonomy and governance systems in specialised and military healthcare institutions that influence the responsiveness to reforms. The present study did not compare the effectiveness across different institutional types of ownership, but such variance across organisations shapes the effectiveness of organisational abilities and implementation of reform. Research on the ownership type of hospitals, as a comparative or moderating institutional factor, should thus be investigated in the future.
CONCLUSION
This research contributes to the literature by demonstrating that patient-centred service quality in the healthcare sector of Saudi Arabia cannot be conceptualised on an isolated managerial basis but rather through a capability-oriented, reform-based approach. In terms of practical contributions, the results show that the concepts of Talent Management and Total Quality Management can be seen as strategic organisational facilitators, with predictive relevance that is heavily reinforced in the structural context of Vision 2030 Healthcare Reform. Workforce capabilities and quality systems can be more institutionally coherent when incorporated into a nationally coordinated governance transformation rather than operating independently. Subsequently, to establish sustainable patient-centred excellence in Saudi healthcare, the harmonisation of the human capital approach with quality governance and macro-level reform architecture is needed. The theoretical contribution demonstrates that adding the dimensions of Talent Management and TQM together with perceived Vision 2030 reform are able to amplify institutional and capability views, to account for contingent effects in healthcare transformation. This study offers practical advice to Saudi healthcare stakeholders to ensure that workforce planning and systems for quality and service delivery are aligned with reform-based governance to achieve positive patient- centred results.
The present study also possesses several methodological shortcomings that must be critically pointed out. First, since the research is cross-sectional, it is not possible to draw causal or temporal inferences from the results regarding the relationship between Talent Management, TQM, healthcare reform and perceived patient-centred service quality. Secondly, having assessed data with the nurse perspective only, there is likely to be perceptual bias and Common Method Bias (CMB). Though Harman’s single-factor test and full collinearity evaluations showed no major statistical problem, practical remedies comprising anonymity of respondents, confidentiality assurance, were also employed to minimise response bias as well as social desirability bias. However, observers still be subject to the influence of using perceptual measures on the strength of observed relationships. Furthermore, patient-centred service quality was measured by the perspective of nurses and not by experiences of patients or objective healthcare measures, which does not always accurately reflect patients’ outcomes. In addition, the findings of the study may not be generalised in terms of the external context, as it focuses on Saudi Arabia, which has a different institutional and governance context from other healthcare systems. Future research with longitudinal and multi-source design is needed, along with objective healthcare performance data and patient feedback, and comparative cross-country studies with enhanced causal inference, methodological strength and external validity.
IMPLICATIONS
The results have specific policy implications for policymakers and hospital administrators involved in the transformation of healthcare in Saudi Arabia. For policymakers, the findings indicate that Vision 2030 programmes should be tailored to align workforce capability building with institutional quality systems by incorporating talent management indicators into national healthcare performance systems. Theoretically, the research develops an integrated perspective of capability, in which talent management accumulates human capital, TQM instils operational practices, and reform governance aligns these capabilities to produce better service quality outcomes. Integrating talent management and indicators of quality performance in national accreditation frameworks and connection to performance-based funding should be a focus in healthcare regulators in the Saudi healthcare organisations to build accountability for healthcare institutions. The vision 2030 quality KPIs should be included on departmental dashboards, clinical audit systems and workforce evaluations to ensure measurable alignment between the vision 2030 goals and the way health services are delivered. In addition, cross-functional governance committees should be established in healthcare organisations to oversee workforce capability, patient safety indicators, digital health use and the ongoing enhancement of quality improvement practices to strengthen the delivery of patient-centred services and institutional performance in the context of health system reforms.
LIST OF ABBREVIATIONS
| AVE | = | Average Variance Extracted |
| CMB | = | Common Method Bias |
| HTMT | = | Heterotrait-Monotrait Ratio |
| PLS-SEM | = | Partial Least Squares Structural Equation Modelling |
| RBV | = | Resource Based View |
| TQM | = | Total Quality Management |
| VIF | = | Variance Inflation Factor |
| VRIN | = | Valuable, Rare, Inimitable, and Irreplaceable Resources |
AUTHOR’S CONTRIBUTION
Q.F.A.A. contributed to the design and implementation of the study. E.A.A.A., H.M.A.A., H.J.H.A. contributed to the analysis of the results and the writing of the manuscript.
ETHICAL APPROVAL & INFORMED CONSENT
All procedures were carried out in accordance with institutional research ethics committee guidelines and Declaration of Helsinki. Informed consent was obtained from all participants. To ensure participant protection, all data were fully anonymized at the point of collection, and no personal or identifiable data was recorded.
AVAILABILITY OF DATA AND MATERIALS
The data will be made available on reasonable request by contacting the corresponding author [Q.F.A.A.].
FUNDING
None.
CONFLICT OF INTEREST
The author declares that there is no conflict of interest regarding the publication of this article.
ACKNOWLEDGEMENTS
Declared none.
DECLARATION OF AI
During the preparation of this work the authors used ChatGPT for editing purposes. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
APPENDIX A
Demographic Factors
- What is your gender?
- Male
- Female
- Prefer not to say
- What is your age group?
- Below 25
- 25–34
- 35–44
- 45–54
- 55 and above
- What is your highest educational qualification?
- Secondary
- Diploma
- Bachelor’s
- Master’s
- Doctorate
- What best describes your current job role?
- Operational/Frontline
- Supervisory
- Managerial
- Senior Management
- How many years of total experience do you have in this industry?
- Less than 3 years
- 3–5 years
- 6–10 years
- More than 10 years
- Which hospital type you work in?
- Public government hospital
- Private hospital
- Military / Specialised government hospital
- Region, where the hospital is located?
- Central
- Eastern
- Western
Survey Questionnaire
| Variable | Question Statement | SD (1) | D (2) | N (3) | A (4) | SA (5) |
| Talent Management Practices | 1. Talent management practices help identify and develop employees who contribute to high-quality patient care. | ☐ | ☐ | ☐ | ☐ | ☐ |
| 2. The organisation’s focus on talent management has enhanced patient-centred care delivery. | ☐ | ☐ | ☐ | ☐ | ☐ | |
| 3. Talent management strategies align with the goal of improving patient outcomes. | ☐ | ☐ | ☐ | ☐ | ☐ | |
| Total Quality Management (TQM) | 1. TQM practices are effective in improving the overall quality of patient care. | ☐ | ☐ | ☐ | ☐ | ☐ |
| 2. The organisation’s commitment to TQM enhances patient satisfaction. | ☐ | ☐ | ☐ | ☐ | ☐ | |
| 3. TQM practices are integrated into daily work processes to improve patient care. | ☐ | ☐ | ☐ | ☐ | ☐ | |
| Vision 2030 Healthcare Reform | 1. Vision 2030 healthcare reforms have strengthened patient-centred care practices within my organisation. | ☐ | ☐ | ☐ | ☐ | ☐ |
| 2. Vision 2030 reforms have improved quality management systems in healthcare institutions. | ☐ | ☐ | ☐ | ☐ | ☐ | |
| 3. Vision 2030 initiatives have promoted digital technologies and innovation in healthcare delivery. | ☐ | ☐ | ☐ | ☐ | ☐ | |
| 4. Vision 2030 reforms have enhanced accountability and governance in healthcare services | ☐ | ☐ | ☐ | ☐ | ☐ | |
| 5. Vision 2030 policies have improved training and professional development opportunities for healthcare staff | ☐ | ☐ | ☐ | ☐ | ☐ | |
| 6. Vision 2030 reforms have encouraged greater efficiency and performance monitoring in healthcare organisations | ☐ | ☐ | ☐ | ☐ | ☐ | |
| Patient-Cantered Service Quality | 1. Prioritise patient needs when making care-related decisions. | ☐ | ☐ | ☐ | ☐ | ☐ |
| 2. Deliver care consistently to enhances the patient experience. | ☐ | ☐ | ☐ | ☐ | ☐ | |
| 3. Focus on patient-centred care contributed to improved patient satisfaction. | ☐ | ☐ | ☐ | ☐ | ☐ |
REFERENCES
AboAlsamh, H. (2025). The dark side of international talent management: Exploring the negative effect of talent repatriation on multinational enterprises’ performance with the meditating role of reverse culture shock. AJBMSS-Advance Journal of Business Management and Social Sciences, 1(1).
https://doi.org/10.65080/942npc70.
Adubasim, E. I., Humphrey Uche Amanze, P. D., & Francis, U. O. (2025). Talent Management Practices and Survival of Healthcare Facilities in Nigeria. International Journal of Business Environment & Intelligence, 4(1), 1-18.
https://doi.org/42721590414.
Akdere, M., Top, M., & Tekingündüz, S. (2020). Examining patient perceptions of service quality in Turkish hospitals: The SERVPERF model. Total quality management & business excellence, 31(3-4), 342-352.
https://doi.org/10.1080/14783363.2018.1427501.
Al Issa, H. E., & Abdelsalam, M. K. (2021). Antecedents to leadership: a CB-SEM and PLS-SEM validation.
https://doi.org/10.18280/ijsdp.160801.
Alanezy, F. M., Alharbi, A. S. D., Alenezi, Y. M., Al-harbi, A. H., Alotaibi, S. H., Al-Harbi, S. M., … & Almutairi, W. M. S. (2025). Paramedics At the Core of Emergency Healthcare Transformation in Saudi Arabia: A Systematic Review. The Review of Diabetic Studies, 58-66.
https://doi.org/10.1016/j.jtumed.2025.08.006.
Al-Arabiya. (2023). Saudi Arabia. The Development of The Health Care Sector Returns the Compass of Investments to the Inside. Available from: https://drsartawi.com/en/saudi-arabia-the-development-of-the-health-care-sector-returns-the-compass-of-investments-to-the-inside/.
Alasiri, A. A., & Mohammed, V. (2022). Healthcare transformation in Saudi Arabia: an overview since the launch of vision 2030. Health Services Insights, 15, 11786329221121214.
https://doi.org/10.1177/11786329221121214.
Aldhobaib, M. A. (2025). The new era of the kingdom of Saudi Arabia: key highlights and future research agenda on organisational strategy. Businesses, 5(1), 5.
https://doi.org/10.3390/businesses5010005.
Alfahad, A. H., Alabbas, Y. S., ALabbas, H. S. M., Abukhashbah, T. H., Alabdali, A. A., Alfatieh, Q. M. H., … & Alhazmi, K. M. A. (2024). Evaluating the impact of Saudi vision 2030 on healthcare investment: a comprehensive review of progress and future directions. J Ecohumanism, 3(8), 870-880.
https://doi.org/10.62754/joe.v3i8.4774.
Alharbi, A., Aljuaid, M., Alamri, F. A., Alosaimi, S. N., & Aldeijy, S. (2025). Health sector transformation in Saudi Arabia—The modern healthcare model: A qualitative study among healthcare leaders. Journal of Taibah University Medical Sciences, 20(5), 643-653.
https://doi.org/10.1016/j.jtumed.2025.08.006.
Ali, N., & Dzandu, M. D. (2023). A paradigm shift for medical health care to focus on a service-value approach to achieve greater patient satisfaction. Journal of Health Organisation and Management, 37(2), 133-157.
https://doi.org/10.1108/jhom-06-2022-0180.
Aljehani, N. M., & Al Nawees, F. E. (2025). The current state, challenges, and future directions of artificial intelligence in healthcare in Saudi Arabia: systematic review. Frontiers in Artificial Intelligence, 8, 1518440.
https://doi.org/10.3389/frai.2025.1518440.
Almutairi, B. H. H., Alsaif, W. A. A., Almutairi, M. M. F., Alotaibi, A. O. M., Alqahtani, M. A. M., Aldlafea, A. M. W., … & Alaqeeli, A. M. (2024). The Role of Implementing Total Quality Management in Improving the Performance of Public Hospitals in the Kingdom of Saudi Arabia. Journal of International Crisis and Risk Communication Research, 7(S10), 223.
https://doi.org/10.63278/jicrcr.vi.293.
Al-Saggaf, L., Al-Hadrami, A. H., & Aoun, M. (2024). Healthcare sector in Saudi Arabia: initiatives and challenges. In Achieving sustainable business through AI, technology education and computer science: Volume 1: Computer science, business sustainability, and competitive advantage (pp. 203-214). Cham: Springer Nature Switzerland.
https://doi.org/10.1007/978-3-031-70855-8_18.
Atalıç, H., & Çiçek, H. (2021). Total quality management practices in health care organisations: Perception of health care providers. European Journal of Public Health Studies, 4(2).
https://doi.org/10.46827/ejphs.v4i2.100.
Baharum, H., Ismail, A., Awang, Z., McKenna, L., Ibrahim, R., Mohamed, Z., & Hassan, N. H. (2023). The study adapted instruments based on Confirmatory Factor Analysis (CFA) to validate measurement models of latent constructs. International Journal of Environmental Research and Public Health, 20(4), 2860.
https://doi.org/10.3390/ijerph20042860.
Baistaman, J., Awang, Z., Afthanorhan, A. and Rahim, M.Z.A., (2020). Developing and validating the measurement model for the financial literacy construct using confirmatory factor analysis. Humanities and Social Science Review, 8(2), pp.413-422.
https://doi.org/10.18510/hssr.2020.8247.
Cha, J., Jang, J., & Lee, K. H. (2024). Tapping Into Patient Engagement in Organisational Performance Improvement: A Social Resource-Based View and the Role of Patient and Family Engagement. Authorea Preprints. Available from: https://d197for5662m48.cloudfront.net/documents/publicationstatus/218459/preprint_pdf/fc4efc64e8e8b3f1011425a5a6c8cb73.pdf.
Chen, M. H., Chen, B. H., Shih, H. M., & Wu, M. H. (2020). Evaluation Research on the Implementation of Talent Quality Management System in Medical Institutions. Journal of Economics and Management, 16, 51-67. Available from: https://www.researchgate.net/profile/Bryan-Chen-4/publication/343230519_Evaluation_Research_on_the_Implementation_of_Talent_Quality_Management_System_in_Medical_Institutions/links/5f1e9728a6fdcc9626b6864f/Evaluation-Research-on-the-Implementation-of-Talent-Quality-Management-System-in-Medical-Institutions.pdf.
Dash, G., & Paul, J. (2021). CB-SEM vs PLS-SEM methods for research in social sciences and technology forecasting. Technological forecasting and social change, 173, 121092.
https://doi.org/10.1016/j.techfore.2021.121092.
Dzimbiri, G. L., & Molefi, A. (2021). The impact of talent management on job satisfaction of registered nurses in Malawian public hospitals. SA Journal of Human Resource Management, 19, 9.
https://doi.org/10.4102/sajhrm.v19i0.1513.
Essa, G. T. K. (2025). Internal Auditing and Organizational Culture As Pillars Of It Governance: Evidence from the Saudi Arabian Healthcare Sector Using PLS-SEM.
https://doi.org/10.5281/zenodo.11425209.
Friedel, A. L., Siegel, S., Kirstein, C. F., Gerigk, M., Bingel, U., Diehl, A., … & Kreitschmann-Andermahr, I. (2023, March). Measuring patient experience and patient satisfaction—how are we doing it and why does it matter? A comparison of European and US American approaches. In Healthcare (Vol. 11, No. 6, p. 797).
https://doi.org/10.3390/healthcare11060797.
Graham, B. E., Zaharie, M., & Osoian, C. (2024). Inclusive talent management philosophy, talent management practices and employees’ outcomes. European Journal of Training and Development, 48(5-6), 576-591.
https://doi.org/10.1108/EJTD-12-2022-0138.
Grossu-Leibovica, D., & Kalkis, H. (2023). Total quality management tools and techniques for improving service quality and client satisfaction in the healthcare environment: A qualitative systematic review. Management Science Letters, 13(2), 118-123.
https://doi.org/10.1051/shsconf/202213102009.
Haroun, A., Ayaad, O., Al-Ruzzieh, M. A., & Ayyad, M. (2022). The role of total quality management in improving patient experiences and outcomes. British Journal of Healthcare Management, 28(10), 1-8.
https://doi.org/10.12968/bjhc.2021.0082.
Howard, M. C., Boudreaux, M., & Oglesby, M. (2024). Can Harman’s single-factor test reliably distinguish between research designs? Not in published management studies. European Journal of Work and Organisational Psychology, 33(6), 790-804.
https://doi.org/10.1080/1359432X.2024.2393462.
Irtaimeh, H. J., Al-Azzam, Z. F., & Khaddam, A. A. (2016). Exploring the impact of talent management strategies and service quality on beneficiaries’ satisfaction in Jordan healthcare sector: Provider point of view. International Journal of Management (IJM), 7(7), 23-38. Available from: http://iaeme.com/Home/issue/IJM?Volume=7&Issue=7.
Jinjing, M., & Karia, N. (2024). The impact of talent management on public hospital performance based on knowledge management. Global Business and Management Research, 16(4s), 1089-1102. Available from: https://www.gbmrjournal.com/pdf/v16n4s/V16N4s-68.pdf.
Kero, C. A., & Bogale, A. T. (2023). A Systematic Review of Resource-Based View and Dynamic Capabilities of Firms and Future Research Avenues. International Journal of Sustainable Development & Planning, 18(10).
https://doi.org/10.18280/ijsdp.181016.
Kosiol, J., Fraser, L., Fitzgerald, A., & Radford, K. (2023). Resource-based view: A new strategic perspective for public health service managers. Asia Pacific Journal of Health Management, 18(1), 8-19.
https://doi.org/10.24083/apjhm.v18i1.2053.
Mani, Z. A., & Goniewicz, K. (2024). Transforming healthcare in Saudi Arabia: a comprehensive evaluation of vision 2030’s impact. Sustainability, 16(8), 3277.
https://doi.org/10.3390/su16083277.
Mat, S. T. B. (2025). Empowering Care: The Evolution of Talent Management in Nursing. MEHES JOURNAL, 3(1), 61-70.
https://doi.org/10.5281/zenodo.15105126.
Nilsen, P., Seing, I., Ericsson, C., Birken, S. A., & Schildmeijer, K. (2020). Characteristics of successful changes in health care organisations: an interview study with physicians, registered nurses and assistant nurses. BMC Health Services research, 20(1), 147.
https://doi.org/10.1186/s12913-020-4999-8.
Nkala, B., Mudimu, C., & Mbengwa, A. M. (2021). Human resources for health talent management contribution: A case for health systems strengthening in the public health sector. World Journal of Advanced Research and Reviews, 9(2), 192-201.
https://doi.org/10.30574/wjarr.2021.9.2.0062.
Obilor, E. I. (2023). Convenience and purposive sampling techniques: Are they the same. International Journal of Innovative Social & Science Education Research, 11(1), 1-7. Retrieved from: https://www.researchgate.net/profile/Esezi-Obilor/publication/398681103_Convenience_and_Purposive_Sampling_Techniques_Are_they_the_Same/links/693fe9e8a1fd01798907e406/Convenience-and-Purposive-Sampling-Techniques-Are-they-the-Same.pdf.
Pereira, L., Jerónimo, C., Salgado, A., Dias, Á., Costa, R. L. D., & Gonçalves, R. (2023). Patient centricity as strategy to improve quality of service in healthcare management. International Journal of Healthcare Technology and Management, 20(1), 1-15.
https://doi.org/10.1504/IJHTM.2023.130319.
Rahman, R., & Al-Borie, H. M. (2021). Strengthening the Saudi Arabian healthcare system: role of vision 2030. International Journal of Healthcare Management, 14(4), 1483-1491.
https://doi.org/10.1080/20479700.2020.1788334.
Rasoolimanesh, S. M. (2022). Discriminant validity assessment in PLS-SEM: A comprehensive composite-based approach. Data Analysis Perspectives Journal, 3(2), 1-8. Available from: https://www.researchgate.net/profile/S-Mostafa-Rasoolimanesh/publication/356961783_Discriminant_validity_assessment_in_PLS-SEM_A_comprehensive_composite-based_approach/links/61b465e31d88475981dfde95/Discriminant-validity-assessment-in-PLS-SEM-A-comprehensive-composite-based-approach.pdf.
Rave, J. I. P., Sánchez Figueroa, G. A., & González Echavarría, F. (2022). A scale for measuring healthcare service quality incorporating patient-centred care and using a psychometric analytics framework. Journal of Health Organisation and Management, 36(6), 816-838.
https://doi.org/10.1108/jhom-10-2021-0387.
Salahat, M., Ajouz, M., Hammash, A., Shehadeh, M., Tunsi, W., Jamjoom, Y., … & Al-Sartawi, A. (2023). The nexus of leadership styles and total quality management: enhancing healthcare sector implications through individual readiness to change within decisions sciences framework. Operational Research in Engineering Sciences: Theory and Applications, 6(4).
https://doi.org/10.31181/oresta/060404.
Shehadeh S., K. J., & Bin Ahmad, M. F. (2025). The Impact of Total Quality Management on Healthcare Service Quality in Jordan and UAE: The Moderating Role of Strategic Management. Lex Localis: Journal of Local Self-Government, 23.
https://doi.org/10.52152/802003.
Tajik, O., Golzar, J., & Noor, S. (2025). Purposive sampling. International Journal of Education & Language Studies, 1-9.
https://doi.org/10.22034/ijels.2025.490681.1029.
Tanujaya, B., Prahmana, R. C. I., & Mumu, J. (2022). Likert scale in social sciences research: Problems and difficulties. FWU Journal of Social Sciences, 16(4), 89-101. http://doi.org/10.51709/19951272/Winter2022/7.
Tessema, D. H., Nuhu, J. A., Obeng, H. A., & Assefa, H. K. (2024). The relationship between total quality management, patient satisfaction, service quality, and trust in the healthcare sector: the case of ethiopian public hospitals. Uluslararası Anadolu Sosyal Bilimler Dergisi, 8(1), 164-176.
https://doi.org/10.47525/ulasbid.1402805.
Zafar, N., Hanif, M., Parveen, S., Mushtaq, F., Bano, S., Awaiz, A. D., & Abid, N. (2025). Total Quality Management in Healthcare Setting and Impact on Patient Outcomes and Healthcare Services Standard. Insights-Journal of Health and Rehabilitation Учредители: Health and Research Insights, 3(2), 208-216.
https://doi.org/10.71000/tzmxnz80.
Zaid, A. A., Arqawi, S. M., Mwais, R. M. A., Al Shobaki, M. J., & Abu-Naser, S. S. (2020). The impact of Total quality management and perceived service quality on patient satisfaction and behavior intention in Palestinian healthcare organisations. Technology Reports of Kansai University, 62(03), 221-232. Available from: https://www.researchgate.net/profile/Ahmed-Zaid-2/publication/341043587_The_Impact_of_Total_Quality_Management_and_Perceived_Service_Quality_on_Patient_Satisfaction_and_Behavior_Intention_in_Palestinian_Healthcare_Organisations/links/5eaaac3592851cb26766e00a/The-Impact-of-Total-Quality-Management-and-Perceived-Service-Quality-on-Patient-Satisfaction-and-Behavior-Intention-in-Palestinian-Healthcare-Organisations.pdf.
Zvarimwa, C., & Zimuto, J. (2022). Valuable, rare, inimitable, non-substitutable and exploitable (VRINE) resources on competitive advantage. International Journal of Business & Management Sciences, 8(1), 9-22.
https://doi.org/10.53555/ephbms.v8i1.1915.
Licensed
© 2026 Copyright by the Authors.
Licensed as an open access article using a CC BY 4.0 license.
Article Contents Author Aliza Moiz1, * 1Greenwich University, Karachi, Pakistan Article History: Received: 26 November, 2025 Accepted: 24 April,
Article Contents Author Ishaq Kalanther1, * 1Jubail Industrial College, Jubail Industrial City, Jubail, Kingdom of Saudi Arabia Article History: Received:
Article Contents Author Qasem Faisal A Alhajji1, * , Eyad Abdulaziz Abdullah Asiri1, Hassan Majed A Alyousef1, Hamad Jamal Hamad
Article Contents Author Mirza Abdulaziz Abdrubalrsool Al Qussair1, * Batal Haran Salem Almari1 Nawaf Saud A Aldossary1 1Imam Abdul Rahman
Article Contents Author Imad Ullah1, * , Ibad Ullah1 , Naseer Ullah1 1Faculty of Computing, Riphah International